My Blog

2026-02-18 11:06
Notes From Refuge
Legal Note – Defamation Act 2013 s. 4 Honest Opinion Defence (Public interest and honest opinion). Covert police surveillance is a matter of public interest, particularly when it involves an innocent, vulnerable adult. My observations that I publish in this post are factual and are published in the public interest to push for police accountability. These facts include number plates, dates and logs. Where I express views, they are my honest opinion based on these facts and are protected under the Defamation Act 2013, Section 4.
Trigger Warning: There is a reference in this post to a suicide attempt that some readers may find distressing. If you need support, please call NHS 24 111, option 2 or Samaritans Freephone, 116 123.
Notes From Refuge
 Notes from Refuge: The last few months since I posted my final blog post on here have been indescribable. Utterly terrifying. Since I ended my online campaign on 31st October, I believe that I have been unlawfully stalked, surveilled and hounded by police from North Yorkshire and across the UK.
I am writing notes from refuge in Orkney, where I fled for safety on January 20th, 2026.
Notes from Refuge: The last few months since I posted my final blog post on here have been indescribable. Utterly terrifying. Since I ended my online campaign on 31st October, I believe that I have been unlawfully stalked, surveilled and hounded by police from North Yorkshire and across the UK.
I am writing notes from refuge in Orkney, where I fled for safety on January 20th, 2026.
***What’s Been Happening?***
 After I wrote my last blog post about ‘suspected’ state surveillance, (phone tracking and CCTV tracking) my suspicions turned into a full-blown reality of unrelenting harassment and stalking by North Yorkshire Police. They have treated me like I’m a spy or terrorist, not the vulnerable adult who needs help and protection. It has been a vicious oversight by those in power – an unforgivable state overreach that has broken me.
The surveillance that I have experienced by North Yorkshire Police started in mid-November, just after I published my final blog post on here and when I had gone visibly quiet on social media – when they knew I’d stopped speaking.
After I wrote my last blog post about ‘suspected’ state surveillance, (phone tracking and CCTV tracking) my suspicions turned into a full-blown reality of unrelenting harassment and stalking by North Yorkshire Police. They have treated me like I’m a spy or terrorist, not the vulnerable adult who needs help and protection. It has been a vicious oversight by those in power – an unforgivable state overreach that has broken me.
The surveillance that I have experienced by North Yorkshire Police started in mid-November, just after I published my final blog post on here and when I had gone visibly quiet on social media – when they knew I’d stopped speaking.
Surveillance Log- North Yorkshire

- Intense Police Presence: A North Yorkshire and Humberside police van was circulating around Kirbymoorside, a town where you never ever see police. Each time my bus, the 128, passed through West End Street in Kirby, the police van passed by and spot-checked me.
- This intensified. There were progressively more police vans in Kirbymoorside. Police vans—unheard of in Kirbymoorside—circulated constantly and were spot-checking my 128 bus. Many residents noticed the amount of police because Kirbymoorisde is a town where there is no police presence.
- Night Operations: Every night at 6.00pm and then at 9.00pm an unmarked car with red and white strobe lights flashing drove past my flat in the rural lanes behind the fields. I thought at first that the cars may be farmers, but the patterns were too consistent. It was police monitoring me. This went on for months and happened even on Sunday evenings.
- Plain Clothed Officers: There were plainclothes officers in cars waiting at the end of my drive. This was particularly noticeable on December 18th, 2025, at 12.10pm.
- Stalking and Visual Interception: Then the stalking started. There were two police cars positioned every night in Kirbymoorisde at the bus stop on Market Place and outside the Memorial Hall from 6.00pm.
- Recorded Incident: January 16th, 2026 I took the 128 bus at 12.45pm to Scarborough to run errands. A police van drove by and spot-checked me at Kirby. At 18.00 when I returned, there was a police van parked at the bus stop on Market Place in Kirbymoorside, the last lit stop before my stop. The officer leant forward to look at the passengers, and then he extinguished the interior light after visually confirming my presence, with no interaction or policing purpose explained. Beyond the night strobes, this was overt stalking.
- Helicopter Monitoring: The same night, there were helicopters circulating over the area where I live.

Orkney
 I felt hemmed in. The police presence was suffocating and terrifying. I thought I was going to be arrested, even though I didn’t know what for. I was so frightened. So, I packed up my flat. I packed a suitcase, and I left. My stuff is still there because I am still paying rent on the property, but I packed a suitcase and fled.
I wanted to leave the mainland because I thought that I’d be safer on an island. I felt pulled by the vast coastal vistas and space of the Orkney Isles. The spirituality of the standing stones in the Ring of Brodgar, the images of the cliffs of Yesnaby, Earl’s Palace in Birsay, and the unique wildlife presence on the island – all felt like a refuge away from police vans and strobing lights.
However, Orkney has not turned out to be the refuge I had hoped for. Police have followed me here. As soon as North Yorkshire police saw I was not at my flat (during their night ops), they clearly entered me into a national police/ intelligence database and handed over the surveillance to Police Scotland. I believe police agents followed me to Orkney and agents are surveilling me here. I cannot convey to you the level of terror I am feeling.
I felt hemmed in. The police presence was suffocating and terrifying. I thought I was going to be arrested, even though I didn’t know what for. I was so frightened. So, I packed up my flat. I packed a suitcase, and I left. My stuff is still there because I am still paying rent on the property, but I packed a suitcase and fled.
I wanted to leave the mainland because I thought that I’d be safer on an island. I felt pulled by the vast coastal vistas and space of the Orkney Isles. The spirituality of the standing stones in the Ring of Brodgar, the images of the cliffs of Yesnaby, Earl’s Palace in Birsay, and the unique wildlife presence on the island – all felt like a refuge away from police vans and strobing lights.
However, Orkney has not turned out to be the refuge I had hoped for. Police have followed me here. As soon as North Yorkshire police saw I was not at my flat (during their night ops), they clearly entered me into a national police/ intelligence database and handed over the surveillance to Police Scotland. I believe police agents followed me to Orkney and agents are surveilling me here. I cannot convey to you the level of terror I am feeling.
My journey
 When I left North Yorkshire, I did everything I could to preserve my privacy. I left my iPhone, iPad and laptop at home so there could be no digital trace of me. I bought a small burner phone that resembled the brick phones of the 1990s. No internet usage, just texts and phone calls. Digital blackout.
I stayed under the radar as much as I could. I took the train to Morpeth and spent two days in a family-run hostel in rural Wooler, where there were owners on site. My journey from Wooler was as safe as it could be. I took taxis all the way to Edinburgh (it cost me a fortune,) with a one-night stopover in a hotel in Duns.
When I left North Yorkshire, I did everything I could to preserve my privacy. I left my iPhone, iPad and laptop at home so there could be no digital trace of me. I bought a small burner phone that resembled the brick phones of the 1990s. No internet usage, just texts and phone calls. Digital blackout.
I stayed under the radar as much as I could. I took the train to Morpeth and spent two days in a family-run hostel in rural Wooler, where there were owners on site. My journey from Wooler was as safe as it could be. I took taxis all the way to Edinburgh (it cost me a fortune,) with a one-night stopover in a hotel in Duns.
Surveillance in Scotland-
Incident Log
 I became visible on CCTV in Edinburgh. That’s when intelligence saw me. I took a City Link bus from Edinburgh to Inverness. The first suspicious activity related to surveillance happened on my journey on the X99 from Inverness to Thurso.
I became visible on CCTV in Edinburgh. That’s when intelligence saw me. I took a City Link bus from Edinburgh to Inverness. The first suspicious activity related to surveillance happened on my journey on the X99 from Inverness to Thurso.
- Friday, January 23rd: deep in the rural landscape of Caithness, on the rocky coastal roads, there was a marked police car at a bus stop when we stopped. I noted it was unusual to see a police car positioned at a bus stop so rurally.
- When I alighted the X99 at Thurso, there was an unmarked black car with flashing red and white strobes at the bus stop. The car waited as I alighted and then followed me to my hotel, The Inn at Y-Not.
- Saturday 24th January, 8.00am: This was the peak of my terror levels. I was having breakfast at my hotel, and a black car pulled up outside my hotel, opposite Lidl, and sat positioned there for an hour with its headlights on. That car followed me to the ferry port at Scrabster.
The Ferry Crossing
- January 24th: Ferry Crossing, MV Hamnavoe Ferry: His car sat at the terminal. His car had a SACRO sticker in the window (a criminal justice organisation in Edinburgh which protects communities from crime and has contracts with the police. North Yorkshire Police potentially contracted SACRO to follow me) It was a black Audi car. His registration number was M24 RDO. At 11.30am, a man wearing a tracksuit and woolly hat walked into the departure lounge. He had no luggage, only an iPad. He sat down, stared at me, and wrote a note on his iPad. I knew he was a police officer or someone official. He stood out like a sore thumb.
- January 24th, 2026, Ferry Arrival: At Stromness, Orkney, the man followed me off the Hamnavoe ferry. He was carrying no luggage. That was noticeable. I stopped to let him pass me by, but he stood by the ferry and watched me walk to the car, where a lady who was housing me for the week was waiting for me.
Surveillance Log – Orkney

- 25th January: 9.00am outside my rented flat in Stromness, I saw the man walking down the high street, looking at me, and then again, I saw him walking past my window early morning at 7.00am on Monday 26th January. He’d clocked where I was staying.
- 27th January/Wednesday 28th January: A black Toyota Prius (Reg: YT61 EUZ) was parked up outside my flat in Stromness with two boat tickets visible on the dash. Two men from the car walked into the block of flats directly opposite where I was staying. Later that day, a huge estate car with “Dunnets of Caithness” on the registration plate parked behind the Toyota Prius. (Caithness is where the intel/police followed me from.)
- 28th January: I felt threatened by these cars. I went to stay at Browns Hostel for the night in Stromness. The black Toyota Prius was driving up and down the street that night appearing to look for me.
- 31st January: I moved to a different property. The landlord drove me to a self-catering cottage I rented in Finstown, where I stayed for a week. I arrived at 1.00pm. At 3.00pm, a man with a woolly hat from the boat and wearing black waterproofs was peering through my sitting-room window.
- 1st February: At 3.00am, I heard men’s voices outside the bedroom window.
- 4th February: The man with the woolly hat and tracksuit from the boat followed me into Magnus Café Kirkwall, was staring at me and looked like he wanted to talk to me, but he didn’t.
- 5th February: An unrecognised man wearing a suit followed me from the library to the Citizens Advice Bureau in Kirkwall. When I came out, he was standing outside, making notes on an iPad.
- Police Vans: 12th February 10:00am en route to Kirkwall library: A police van slows as they pass me; two officers laugh pointedly. I felt unnerved by this.
- 13th February 10.00am, Same van with the same officers as yesterday passed me again on Junction Road as I walked to the library and slowed as they passed me.
Library Surveillance
- 9th February: At Kirkwall library, a man matching ‘one of them’ description, (well dressed and official) was sitting in library foyer, laptop on home screen (not working), staring directly at me while I got a cigarette. Fear logged with library staff at 11.20am. Man left soon after.
- Feb 10th 3:15pm, Kirkwall Library – A bald headed man in a brown jumper, jeans, brown shoes, tan suede jacket over adjacent chair (seen multiple times) – was sitting at a desktop directly opposite me displaying MY BLOG IMAGES/NYP images and scans – Writing in LONG HANDWRITTEN LOG when spotted – Switched to cartoons after I passed = monitoring target. Terrifying.
- Feb 13th 2.00pm: Same bald headed man from 10th February came into Kirkwall library again and this time sat directly opposite me- too close. He was wearing blue jeans and a blue shirt this time and was looking at cartoons on desktop. Odd- middle aged man, clearly wealthy, looking at cartoons on library desktop. I logged fear with staff.
- Feb 16th and Feb 17th: The same man returned to Kirkwall library, at 2-4pm. He sat at computer facing the wall. He seems to be the main agent allocated to Kirkwall librray.
Suspicious Residential Stalking
Orkney council have placed me in Peedie Hostel, Kirkwall for temporary housing for four weeks until March 3rd. Over the past week, clear patterns indicate undercover police stalking is happening at the hostel. The evidence suggests that this is likely. I checked in on Saturday 7th February.- 8th February, 8.00pm: a man checked into Peedie Hostel, Kirkwall, claiming to be ‘touring’ and was seen on Monday, 9th February, driving off in high vis on a BMW motorbike at 9.00am (reg: RF21/RE21 OPX). As I left my bothy at Peedie Hostel on the morning of 9th February, someone opened and then slammed shut the hostel door as I passed. Appeared they wanted to see me but didn’t want to be seen.
- Feb 8th-9th pattern: English ‘touring’ guest arrives the night after I check in → Mon 9th 9am BMW bike RF21/RE21 OPX alley → door slams as I pass reception → 11am library stare (blank laptop). Pre-guest: quiet. Post-guest: suspicious targeting.
- BMW status on 11th February: Now covered and stationary at Peedie Hostel (odd for a “tourer”—and a BMW vehicle is out of place at a hostel, where homeless people are temporarily placed).
- 11th February, 8.00pm: The house opposite my bothy had been empty since 7th February, but it was suddenly occupied at 8.00pm by a man wearing jeans/black waterproof with a strong Orcadian accent, who checked in on his own. The owner and the man were talking outside my door. The owner said to him, “The girl is staying there.” He was up all night moving—possible operational surveillance, not a normal guest for a hostel. Unconfirmed but possibly a local asset used to closely monitor me.
- Rotation signs, 13 February: The situation with these two men is becoming more suspicious as the days unfold. Firstly, a well-dressed middle-aged man, alone in a hostel with a BMW bike, looks out of place. Secondly, their movements seem to indicate a possible rotation watch. Yesterday, I arrived back at the hostel at 6.00pm. The house light was on, man. A, (Orcadian man) is at home. Ten mins later, the light is off, he goes out, and the BMW arrives back – man B (BMW rider) returns. Thirdly, man A, (Orcadian man) is up all night in the ‘hoose’ until 6.00am, turning water on and off and doing washing, and then he crashes at 6.00am, which suggests possible night duty watch.
- 13 Feb-15 Feb: Audio Cover-Night Watch: Nightly audio cover from Man A’s hoose. Over the weekend, all through the night, there were incessant water flushing sounds coming from the ‘hoose’ where man A, (Orcadian man) is staying. At 3.00am and 4.00am, there were incessant sounds of spin cycles on a washing machine, which was obviously being used to cover for audio updates or conversations he didn’t want to be heard. There were none of these sounds when the man was out in the day or before he arrived.
- 16th February: Audio Team Installed – Operation Escalation: At 6.00am I opened my door and looked up at the ‘hoose’ window. The light was on. The man obviously saw I clocked him. The flushing sounds and spin cycles stopped immediately. At 10.00am, I was going out to the taxi. An Italian man who I had not seen before came out of the main hostel building, (black and white checkered trousers.) He said ‘hello’, and he was walking towards the ‘hoose’ as if he was looking for someone there. He was carrying a large zip bag concealing what looked like a shotgun microphone. The new Italian man saw that I was staring at him. He looked at me suspiciously as he waited at the ‘hoose’.
Live Tracking
- Since I saw the officer deliver the shotgun microphone to the ‘hoose’ at Peedie Hostel on 16th February, it seems that my movements are now being recorded. I’m too frightened to use my phone to call Samaritans or Breathing Space for support – for fear of being monitored. I’d have more freedom in a prison cell.
- The constant water flushing and washing machine on spin cycles at 3.00am continues from the hoose where man A is staying. It is, I believe an audio cover for updates back to the team and other conversations. This is classic behaviour for covering covert operations like this. It is starving me of sleep. I believe that it is necessary to request from the owner of Peedie hostel a review of the water and electric bill for the duration that man A has been in the ‘hoose’. That will serve as evidence of unusual electric and water use.
Assessment
This is a serious surveillance operation that is going on. I feel sick with terror. I am shaking as I write this, nauseous from sleepless nights listening to man A pace relentlessly and cycle the water on/off and new developments every five minutes. It looks more than 90% likely that I am being stalked by police at Peedie Hostel. They are on site. I am terrified for my well-being and safety. I live in constant fear of arrest. This is disgusting and coercive. This RIPA-breaching operation under a civilian roof terrorises a vulnerable adult in council care. I demand IOPC probe + CCTV/guest logs release. These reported incidents in Scotland suggest that North Yorkshire Police have handed over this operation to Police Scotland/national surveillance. I am being surveilled by Police Scotland or a surveillance unit nationally, who have no warrant or safeguarding order. This is a violation of my human right to privacy, (ECHR 8) and my human right to life, (ECHR 2). The most recent incidents – library surveillance on 10th Feb and property stalking – echo the NDEDIU (National Domestic Extremism and Disorder Intelligence Unit (SDS successor) -style coordination and intimidation, given its close proximity to me and the rotation of agents. The NDEDIU is the direct SDS successor, targeting campaigns through undercover proximity intimidation. The Orkney leg of this surveillance seems to be an undercover operation to closely monitor me. I am terrified.Orkney Council
Feb 10th: Orkney Council kindly agreed to house me in temporary accommodation (Kirkwall hostel) for four weeks until March 3rd. However, they have refused permanent housing despite documented NYP/Police Scotland surveillance (Peedie CCTV, SACRO M24 ROO/RDO, library logs). Despite knowing that I fled my property in Yorkshire due to police harassment, Orkney Council claim I am not homeless because ‘I have a secure tenancy, and it is reasonable for me to return to Yorkshire.’ They also falsely stated I ‘refused’ to give them permission to investigate the issues or to clarify my housing history. This is untrue. I did not refuse. They have not done any welfare checks despite my stated suicidal risk. I told them I was terrified and requested refuge at Women’s Aid, but they refused. The close surveillance continues: the man opposite pacing all night, repeatedly turning water on/off until collapsing. New man arrives on the scene. I felt physically sick with terror, and unable to sleep. The property has CCTV, so I feel a bit safer than in an isolated cottage. However, even here at the hostel, where I felt a measure of safety with its CCTV presence, unease has followed, (see section above.) Something doesn’t feel right in these details. The fear persists. No protection or help from council.My Feelings
I believe that none of this surveillance is lawful. North Yorkshire Police, Police Scotland or any force have a safeguarding order over me or warrant to surveil me. I am a law abiding, peaceful citizen. I have no criminal convictions and I am not a threat to national security or public safety. In order to surveil someone legally in UK, they have to be one of those. My campaign content also fell within protected speech, (ECHR 10.) I feel terrified and worn down. My future is uncertain. However, this is what disgusts me about this surveillance operation that North Yorkshire Police have launched. Firstly, they waited until I had gone digitally silent before they pounced. They waited until I published my final social media post and blog posts. I find this sinister and cowardly. Secondly, in only April 2025, they served a Public Protection Notice (PPN) on North Yorkshire County Council asking them to safeguard me and support me, which NYCC ignored. North Yorkshire Police also carried out a forced entry welfare check on my property in February 2025 after my suicide attempt. They therefore knew I am a vulnerable adult in crisis. To stalk and terrorize a vulnerable adult in this way is criminal, when they are not a threat to national security or public safety. Government bodies have silenced and persecuted me for whistleblowing about NHS failings when the state knows that I am deeply vulnerable. This begs the question – most seriously – whether the United Kingdom really is a liberal democracy because, in my humble view, this conduct by government bodies and state agents is the conduct of a nasty totalitarian state. It’s most certainly not the behaviour of a country that supports free speech and the human rights of its citizens.What Actions Have I taken?
 I have contacted numerous human rights lawyers across the UK – the crème de la crème in police misconduct – asking for their help (Deighton Pierce Glynn, Hodge Jones Allen, Russell Cooke and Rahmen Ravelli.) Many have not responded at all, and others have declined to help me because they say they don’t ‘have capacity’ or because there is a ‘conflict of interest’. It has been heartbreaking to receive these rejections, particularly whilst I am being followed by police, being stalked at bus stops and being hemmed in by nighttime drive-bys. I concluded it’s a closed loop – the system, that is. A gated system. I stopped reaching out.
I’ve contacted 20-plus global outlets with tips about fleeing from North Yorkshire due to police surveillance and about the state-mandated censorship of my campaign by the National Security Online Security Team (NSOIT,) but sadly I have had zero response. Perhaps they don’t believe me. I mean, who would? It’s a James Bond movie. But I’m not James Bond.
I submitted a record of these criminal allegations about police officers to the Crown Office Procurator Fiscal Service (COPFS) in Kirkwall, Orkney, on January 29th, 2026. I did not get a response from them. The Procurator Fiscal said she would get back to me, but I did not hear from her. On the same day that I submitted my complaint to the COPFS, I also signaled this to the European Court of Human Rights in Strasbourg.
I have reached out to Advocacy in Orkney, who said they would refer my case to a solicitor and get back to me but I have not heard back from them.
I have contacted numerous human rights lawyers across the UK – the crème de la crème in police misconduct – asking for their help (Deighton Pierce Glynn, Hodge Jones Allen, Russell Cooke and Rahmen Ravelli.) Many have not responded at all, and others have declined to help me because they say they don’t ‘have capacity’ or because there is a ‘conflict of interest’. It has been heartbreaking to receive these rejections, particularly whilst I am being followed by police, being stalked at bus stops and being hemmed in by nighttime drive-bys. I concluded it’s a closed loop – the system, that is. A gated system. I stopped reaching out.
I’ve contacted 20-plus global outlets with tips about fleeing from North Yorkshire due to police surveillance and about the state-mandated censorship of my campaign by the National Security Online Security Team (NSOIT,) but sadly I have had zero response. Perhaps they don’t believe me. I mean, who would? It’s a James Bond movie. But I’m not James Bond.
I submitted a record of these criminal allegations about police officers to the Crown Office Procurator Fiscal Service (COPFS) in Kirkwall, Orkney, on January 29th, 2026. I did not get a response from them. The Procurator Fiscal said she would get back to me, but I did not hear from her. On the same day that I submitted my complaint to the COPFS, I also signaled this to the European Court of Human Rights in Strasbourg.
I have reached out to Advocacy in Orkney, who said they would refer my case to a solicitor and get back to me but I have not heard back from them.
A Closed System
 I have recorded. I have warned, and I have tried to seek accountability, even while homeless in Orkney, but nothing will yield. The stalking continues.
I am effectively homeless and terrified, and I see no way out apart from seeking asylum in Europe, which I don’t have the energy to do. The state has hounded me because it is, I believe, terrified of what I revealed during my campaign. The reality of what I exposed was catastrophic in their eyes to the reputation of the NHS trusts I named, so hounding and silencing me has been their solution. Cover it up. None of this is about me, my safety or well-being. This is about reputational management and trying to contain a potential NHS scandal.
I have recorded. I have warned, and I have tried to seek accountability, even while homeless in Orkney, but nothing will yield. The stalking continues.
I am effectively homeless and terrified, and I see no way out apart from seeking asylum in Europe, which I don’t have the energy to do. The state has hounded me because it is, I believe, terrified of what I revealed during my campaign. The reality of what I exposed was catastrophic in their eyes to the reputation of the NHS trusts I named, so hounding and silencing me has been their solution. Cover it up. None of this is about me, my safety or well-being. This is about reputational management and trying to contain a potential NHS scandal.
Second Suicide Attempt
Following the pressures of on-site police surveillance at Peedie Hostel, I made another suicide attempt on Wednesday night, February 18th, 2026. I took an overdose. Ten minutes after I took the overdose after, and whilst still awake, the police broke in, indicating that they are live tracking me. An ambulance took me to Balfour Hospital, where I spent the night and was revived. In the morning, the mental health team came to see me and didn’t even ask how I was. They offered me no support, no follow-up care and no support plan. They discharged me.
Balfour Hospital discharged me on Friday, 20th February, without even giving me a discharge summary. I left with no paperwork. Can someone please tell me what the hell I am supposed to do? There is no avenue of help. There’s been no welfare check since Friday from the police or the council. This is state persecution. I have never felt this alone or frightened. The coldness from the teams at Balfour Hospital was chilling. Not even a ‘how are you?’ The most torturous aspect is that when I try and set myself free from this oppressive surveillance, police break in and stop me. They revive me and leave me with no safeguarding or support; imprisoned and watched. The mental health team at Balfour Hospital did not even do an assessment. They saw me for a total of ten minutes before letting me go. Why don’t they let me go and be free?Unequivocal Evidence of Live Audio Tracking
The fact that the police broke into my bothy 10 minutes after I had taken my overdose proves that they are tracking me live via audio equipment from the ‘hoose’ where man A is residing. After I took the tablets, I did not call for help; or call 999. I made no cry for help. I just lay there quietly and waited to go to sleep, and before I knew it, the police were there. The shotgun mic that I saw the Italian man deliver to the hoose on 16th February at 10.00am is clearly picking up minuscule sounds from my room, including me drinking water and opening tablet packets. This is intrusive surveillance at its most extreme.
To Prime Minister Sir Keir Starmer:

MP Portraits Project in The Reasons Room.
What I Ask of You
 If you are reading this, I may no longer be able to speak for myself, or I may be at the end of my strength. But what I have done is not nothing. I have tried to document a pattern of surveillance, harassment, and possible misuse of police powers in Orkney, linked to North Yorkshire Police and wider structures. My actions include: I have handed evidence to the Crown Office and Procurator Fiscal Service in Kirkwall and Edinburgh, and I have signalled this matter to the European Court of Human Rights. I have also shared material with journalists and media outlets across Europe and the US.
I am scared, exhausted, and pushed to the edge—but I have tried to act with as much clarity and care as I could under pressure. If I am no longer able to continue this fight, I want the following to be known:
If you are reading this, I may no longer be able to speak for myself, or I may be at the end of my strength. But what I have done is not nothing. I have tried to document a pattern of surveillance, harassment, and possible misuse of police powers in Orkney, linked to North Yorkshire Police and wider structures. My actions include: I have handed evidence to the Crown Office and Procurator Fiscal Service in Kirkwall and Edinburgh, and I have signalled this matter to the European Court of Human Rights. I have also shared material with journalists and media outlets across Europe and the US.
I am scared, exhausted, and pushed to the edge—but I have tried to act with as much clarity and care as I could under pressure. If I am no longer able to continue this fight, I want the following to be known:
- I handed a dossier of evidence to Sue Foard, Procurator Fiscal, at Kirkwall Sheriff Court on 29th January, 2026.
- I have sent hard copies to COPFS in Edinburgh and to the European Court of Human Rights in Strasbourg.
- I have emailed COPFS (enquirypoint@copfs.gov.ukand pfokirkwall@copfs.gov.uk) confirming this.
- I have also shared material with multiple investigative outlets and journalists, and I have kept a personal archive of documents, screenshots, and notes.
- I’ve contacted top-tier human rights law firms and pleaded with heads of departments for help to no avail.
- I’ve reached out to advocacy agencies.
Please Ask These Questions!
I will keep doing my best but if I disappear or am arrested, please treat this as a red flag. Do not assume that the system has acted fairly just because it claims to have done so. Ask:- Why did Penny Dash, the CQC, the DHSC and 40 MPs ignore four of my public pleas for help during my campaign?
- Why did NSOIT or a government body order search engines and platforms to suppress the visibility of my campaign when my content fell within protected speech?
- Why did the platforms comply with an unlawful directive that violated my human right to expression, (ECHR 10)?
- Why did North Yorkshire Police start this surveillance operation with no warrant or safeguarding order to do so?
- Why did North Yorkshire police hand over my case to national intelligence/Police Scotland so that police followed me to Orkney?
- Why are plain clothed agents following me into libraries, cafes, the CAB, following me on boats and stalking me at my accommodation via audio tracking and onsite agents? Who signed this undercover operation off?
- What links exist between North Yorkshire Police and the surveillance I experienced in Scotland? How is this intel data sharing legal?
- What happened to the dossier I handed in to the COPFS recording this?
- What did COPFS do with it?
- Has the COPFS greenlighted the escalation of this operation? Did they know about it and not act?
On a Larger scale, Please Ask:

- How can this level of state overreach go unrecorded or unregulated?
- How can someone survive twelve years of systemic neglect, four months of regulatory silence following a benign led campaign, state-mandated censorship and police surveillance and harassment without help?
- Who can survive that? Could you?
Final Update: 28 February, 2026
Discovering Multiple Unauthorized Proton Mail Logins
The most alarming update to my surveillance log is that I have just discovered that my Proton Mail session management reveals multiple unauthorized webmail and web account logins spanning weeks, confirming that stalkers have potentially been accessing the emails that I have been sending to the press and to law firms. There are multiple logins from different web accounts (different from mine) in my encrypted Proton Mail account, indicating that my Proton Mail account is being actively accessed rather than a single failed breach attempt. There is evidence in my Proton Mail account of over five different web accounts logging in at different points to my account since I have been in Orkney. This indicates that there has possibly been a team of people rotating access to my emails via the library. This is where I have been spending my days sending emails to human rights lawyers seeking help and sending tips to press outlets about what I am experiencing. This is the most intrusive aspect of this surveillance operation. It actively violates data protection laws and The Computer Misuse Act, not just human rights laws. The entry point into my realisation was after I took my overdose on 18 February; I asked the nurse at Balfour Hospital why the police broke in so quickly after I had taken the overdose. The nurse innocently told me, ‘They saw your emails.’ This is what has caused me to scan my Proton Mail account for alien logins. Due to the extreme seriousness of ongoing threats documented above (multiple unauthorized Proton Mail sessions confirming state-level email surveillance), this serves as my final blog post and evidence update for now. All server-side logs are preserved with Proton, which anyone can subpoena directly.Reform Needed
I can only end by asking how on earth a patient who was simply asking for help and accountability online has ended up being hounded in this intrusive way and having her privacy stripped away from her this significantly. I hope that my disclosures serve as a vital catalyst for urgent reform regarding the privacy of citizens, data protection and the reigning in of surveillance police powers. Thank you. Photo Credits: Prime Minister Sir Keir Starmer Official Portrait. Photo: Simon Dawson / No 10 Downing Street / Wikimedia Commons (Open Government Licence v3.0)* Maxwell Andrews, Mark Foster, David Bayliss, Saul Brotheridge, Omar, Bruce Kunkel and Jamie Street on Unsplash. Watford Media, J Costa, Anna Tarazevich, Markus Winkler and Cottonbro on Pexels.
2025-11-27 08:04
On State Surveillance and The Violation of my Human Rights
Disclaimer: The post titled “On State Surveillance” does not intend to attack government bodies. This post is based on lived experience, and it raises serious concerns in the public interest about human rights violations.
This post is part of a civic testimony documenting concerns over surveillance and institutional suppression. It constitutes protected speech under Article 10 of the European Convention on Human Rights and relevant international law.
This content does not promote hatred, violence, or discrimination. Any interpretation to the contrary is a misrepresentation of its intent and content. It forms part of a documented record of lived experience and systemic obstruction.
Summary

My previous post documented my concerns regarding the digital suppression and censorship of my campaign content by, I believe the UK Home Office. This post discusses the possible state surveillance that I think I am under by either the police or the Home Office. Since my campaign ended on October 31st due to what I believe was digital suppression and censorship, I have become deeply concerned that my phone may be subject to unauthorised tracking or “pinging.”
This post also explains that for reasons of personal safety, I am drawing this blog to a close for now, until this censorship and state surveillance that I suspect is happening has subsided. I don’t feel safe continuing to publish online content under these conditions.
Containment

I have been spending most of my time up in Northumberland. I love it up there and I feel safer there. Being in Northumberland provides me with physical distance from North Yorkshire, the location where I have experienced harm and abuse related to Ampleforth Surgery, North Yorkshire County Council, Tees, Esk and Wear Valley Trust (TEWV,) and potentially North Yorkshire police, (as I think the local police may be involved in the digital suppression of my campaign.)
When I am away from North Yorkshire, I am better able to keep myself safe. I filmed all of my campaign videos from locations in Northumberland. Occasionally I choose other locations to go to, and I have made it public that I spend a lot of time away. I travel lawfully and peacefully on trains or coaches to these places, and I conduct myself lawfully and peacefully when staying in Airbnbs. No homeowners or agencies have complained to me about misbehaviour. I am a peaceful citizen.
Obstruction of Movement

I made plans to travel for a week to Pembroke, South Wales, after my campaign ended on October 31st, 2025. I had booked a coach to leave Leeds at 9.00am on Sunday, 2nd November. On the Saturday 1st November, I called a local taxi firm in Malton, who I have been using for years and who have never denied me a fare before. I asked them if they could collect me at 7.00am to take me to Malton bus station so I could board a bus to Leeds.
The firm told me that they had ‘no availability’ to take me to Leeds ‘and could not take me.’ I found it strange that they were fully booked at 7.00am on a Sunday. 7.00am on Sunday is not a busy time of the week. I found a taxi company in Leeds, whom I booked a fare with. It was scheduled for them to collect me at 7.45am on Sunday. However, on Saturday morning, they phoned me to say they ‘could not take me.’
I don’t know for sure, but I think it is possible that these two denied fares were due to either the police or state agents calling them to tell them not to take me anywhere. It just seemed too random for two firms to deny me fares at that time of day.
No authority currently has any safeguarding orders over me. I am free to travel where I wish. If anyone did tell these taxi firms not to take me to Leeds, then it would constitute possible safeguarding abuse. It also constitutes containment and obstruction. As a result of these denied taxi fares, I had to rebook a train ticket, which was expensive and took me an extra twelve hours of travel.
Human Rights Act –
Article 5: Right to Liberty

If an authority instructed these taxi firms to refuse service to me for travel to Leeds, it could potentially contravene Article 5 of the Human Rights Act, which guarantees the Right to Liberty and Security. This article protects individuals from arbitrary detention or restrictions in movement.
It guarantees that no one can prevent an individual from moving freely without lawful justification. Any restrictions imposed must be proportionate, lawful, and necessary, such as those enacted for public safety or legal proceedings. Restrictions like travel bans, surveillance-based limitations, or coercive monitoring could potentially breach Article 5 if they are not legally justified.
Surveillance – ‘Ping’.

I’m not 100% sure, but I believe it’s possible that the Home Office or the police are using “Ping” to monitor my whereabouts. A ping is a digital signal your phone sends out to connect with nearby cell towers. This signal happens automatically.
Every time your phone pings a tower, it leaves a traceable record of your location. These pings allow mobile networks to monitor your movements across various locations.

Law enforcement and surveillance systems utilise this data to observe individuals. They typically access phone location data through formal legal requests to network providers.
Agencies require warrants or court orders under laws like the Investigatory Powers Act. When a person poses an immediate threat, there are emergency exceptions that allow authorities to access data without prior authorisation. However, unapproved or unofficial access, particularly without a warrant, may be illegal and constitute a serious invasion of privacy.
Police requests for this access to data must be logged and auditable, identify the person and device, and provide justification (such as a legitimate criminal investigation or national security). Under UK law, lawful interception is permitted only with proper legal authority or with oversight from regulatory bodies.

The Human Rights Act, Article 8:
The Right to Private Life

Article 8: Human Rights Act – Right to Privacy.
If the police or state authorities have no warrant or legal basis for accessing this data, tracking my movements and my phone violates Article 8 of the Human Rights Act: The Right to a Private Life. Article 8 states that:
‘Everyone has the right to respect for his private and family life, his home and his correspondence.There shall be no interference by a public authority with the exercise of this right except such as is in accordance with the law and is necessary in a democratic society in the interests of national security, public safety or the economic well-being of the country, for the prevention of disorder or crime’[i]
The right to a private life incorporates the privacy of one’s identity, psychological integrity and one’s communications. This incorporates data and digital presence.
If a provider shared data without logging the request or outside legal channels, it may constitute unlawful surveillance. In summary, unauthorised surveillance, metadata tracking, or suppression of digital testimony – especially if it targets protected speech – may constitute a breach of Article 8.
I am not posing a threat to national security or public safety. Nor am I causing disorder or crime. Therefore, if this surveillance is taking place, it may constitute unlawful surveillance. It is definitley a violation of my human right to privacy.
Reflection

I cannot know for sure if these allegations of state surveillance are true, but I think they are. I also think that authorities are possibly monitoring me via CCTV and facial recognition when I travel through hubs like Leeds, York and Newcastle. The reason that I think they are doing this, is not for concern for my safety, but to contain and watch me due to the controversy of my campaign.
This is not an accusation. However, after my recent trip to Wales, I have reason to believe it could be happening. If it is happening, it would represent a serious violation of Article 8 of the Human Rights Act—the right to privacy, liberty and freedom of movement. This action follows my recent concerns about the digital suppression of my campaign content, a potential violation of Article 10 (Freedom of Expression).
While I have little control over the algorithmic suppression of my campaign content, I do have some control over who can monitor my phone. For that reason, I will now be leaving my mobile phone at home to prevent any possible tracking and surveillance of my movements.
An Act of Protection

I do not intend to cause distress or alarm by leaving my phone at home. It is simply a measure to protect my fundamental right to privacy. I am moving about lawfully and peacefully, and there is no warrant or safeguarding order over me that could necessitate a reason to track my movements.
I also shared this intention publicly on social media: on X, TikTok and You Tube on 10th November, 2025 so that, if my phone stops pinging at cell towers, this is the documented reason.
Coupled with the violation of Article 10 of the Human Rights Act, the right to freedom of expression (which has happened with the digital suppression of my testimony), this potential unlawful state surveillance is a serious impingement of my human rights.
I am therefore calling on the UN special rapporteur on Human Rights to review these patterns.
Final Blog Post

I am terrified by this possible state surveillance. I am frightened for my life and for my safety. My system has gone into a state of ‘freeze’. I have decided to therefore draw this blog to a close for now. I plan to turn my attention to memoir and novel writing: more private creative pursuits, which do not expose me to attack or surveillance by the state.
My Facial Pain will remain live indefinitely. I hope that this website will continue to be a source of information and a resource for readers.
I would like to thank all of the readers who have visited My Facial Pain. Whilst it has not found the reach I had hoped for, for a site that is so detailed, I have been delighted with the steady flow of visitors, so thank you for visiting.
This blog has been a labour of love. It is a body of work that I am deeply proud of. The posts cover such a wide range of topics. I have poured hours of thought and work into creating them. I therefore hope that they will continue to reach as many readers as possible!
It’s a sad note to end on – Silenced by the state and punished for speaking out. This is the reality of the world we live in. Systems do what they have to do to protect their reputations. Even at the expense of a genuine patient in urgent need of help.
It’s tragic, but I trust that you understand why I am having to pull back. It’s for my safety.
Thank you for your support.
Love Felicia X

Footnotes
[i] Human Rights Act, 1998, Article 8, Schedule 1, part 1, www.legislation.gov.uk
Photo Credits: Mike Van Schoonderwart, Marcelo Chagas, Stefan Coders, Imjimmyqian, WdToro, KindelMedia, Pixabay, Brett Sayles and Mart Production on Pexels.

2025-11-27 07:06
On State Mandated Censorship: The Eclipsing of my Voice.
Disclaimer: State-Mandated censorship is not an attack on individuals or government bodies. This post is part of a civic testimony documenting concerns over censorship, institutional suppression and human rights violations. It constitutes protected speech under Article 10 of the European Convention on Human Rights and relevant international law.
This content does not contain misinformation. Nor does it promote hatred, violence, or discrimination. Any interpretation to the contrary is a misrepresentation of its intent and content. It forms part of a documented record of lived experience and systemic obstruction.
Trigger Alert: This post heavily discusses institutional harm and state-level censorship that some readers may find distressing. If you are affected by these issues and need support, please call NHS 111 (option 2) or the Samaritans freephone on 116 123.
Summary

This blog post and campaign video document my deepest heartbreak and shock at what appears to be state-mandated censorship and suppression of my online campaign content. It documents the systemic visibility suppression and metadata blackout of my campaign content following high platform engagement. This post marks the eclipsing of reach and notification silence across digital systems.
This post documents the events that have unfolded since my last post regarding the first stage of the digital suppression of my campaign—a directive that I believe is coming from the central government.
What’s Been Happening?

My previous post outlined my observations regarding the disappearance of numerous links to my campaign posts on X from Google search results. I raised the concern that NHS trusts may be submitting ‘Right to Be Forgotten’ (RTBF) requests to ask that Google remove these links from search engine results. This is what has happened since that discovery.
I believe I have been the victim of state mandated censorship. I believe this suppression originated from the Home Office or Central Government. However, I believe that North Yorkshire Police possibly triggered this suppression. It is my belief that in the final weeks of October, 2025, a government body issued a directive to all social media platforms and search engines to suppress the visibility of my campaign content. The intent appears to have been to sanitise the public record and to shield evidence of institutional failures.
The state mandated directive has resulted in the systematic deindexing, shadow banning, and algorithmic throttling of my testimony across multiple platforms. It has obstructed my ability to seek help, share evidence, and engage with public interest communities. I believe this constitutes a misuse of state power and a violation of my human rights, particularly my right to freedom of expression under Article 10 of the European Convention on Human Rights.
Here is what has happened:
Bing and Yahoo.

The first thing that I discovered regarding this state mandated censorship of my campaign content is that there is a sign under my X profile on Bing and Yahoo which says they are not allowed to crawl my X page.
Until the end of October, 2025, Bing and Yahoo had fully indexed all of my campaign videos from both TikTok and YouTube. However, in the later part of October, they were all removed. There were none of my campaign videos or any of my silent diaries visible on Bing or Yahoo. A central body has clearly forbidden competing search engines from indexing my campaign content.
After I published this video on TikTok and X, Bing and Yahoo reindexed my YouTube videos. However, they have still not reindexed any of my TikTok campaign videos or silent diaries, which have had high engagement.
My vidoes on TikTok have had thousands of views which is why I assume that central governement have disallowed competing search engines from indexing these ones. There is still a sign under my X page saying that Bing are disallowed from crawling it. This indicates that a central government body is still disallowing competing search engines from indexing from my campaign content.
Google De-indexing

I explained in my previous post that in mid October, links to my X campaign posts were disappearring from Google. I thought that NHS trusts had maybe submitted ‘Right to Be Forgotten Requests’ (RTBF) to Google and I thought that this is what was causing the links to my X posts to be de indexed.
Howevere, later developments caused me to think that this was tied to a much larger censorship directive. Until October 20th, 2025, my X profile and latest posts on X have always been highly visible on Google. My X profile and ‘latest posts’ from my X feed have consistently appeared in search results on Google. However, at the same time that Bing and Yahoo had de indexed my campaign videos, Google removed my latest posts from my X on Google search results. They were no longer indexed on Google.
Additionally, Google’s desktop version deindexed my X profile. My X Profile disappeared. Additionally, Google had not indexed my YouTube channel with all my campaign videos, even though I had 1.7k subscribers. My video campaign’s visibility on Google significantly changed as a result of these four incidents.
Algorithmic Throttling

The worst part of this state mandated censorship has been the algorithmic suppression and throttling of my campaign content on YouTube, X and TikTok. It has been heartbreaking.
TikTok
My TikTok account has been a thriving hub during my campaign. My videos have had thousands of views. TikTok has been continually circulating my videos. Every day, the view count increases on my videos. TikTok has been a wonderful experience of solidarity and support.
The support from people has been incredible. I received at least thirty notifications every morning when I woke up, including likes, comments, and reposts of my videos. After enduring this injustice on my own for twelve years, I have experienced a genuine sense of solidarity from those who have expressed true empathy for my plight. It has made me feel less isolated.
However, on the evening of 26th October, my TikTok archive went eerily quiet. This support abruptly stopped. TikTok ceased circulating my videos at the frequencing that they were doing, notifications significantly diminished, and I was digitally cut off from vital support. The view counts on most of my videos froze.
Since October 26th, the view counts on my videos have stayed the same. Now I get one or two notifications every day from select close followers. This indicates that a central body has possibly told TikTok to only show my videos on very few ‘For You’ feeds. These notifications from supporters have stopped because TikTok does not appear to be sharing my videos as they did.
It is so difficult to lose this connection to viewers. I feel bereft of the support and the dynamic impact my content was making. I feel increasingly more alone by the day. What is so heartbreaking about this silencing is that the lack of response from the DHSC to my pleas for help is hard enough. To be then cut off from supporters feels like persecution.
X, formerly Twitter.
The same pattern occurred on X. My reach was throttled, with views dropping to as low as 60 per post. Only a small cluster of loyal followers continued to see my content. Whilst my posts were still on my feed, very few people were seeing them and they were not indexed. This signficantly eclipsed their visibility.
I do not believe that this sudden decline in views and decrease in notifications on platforms is an algorithmic shift. I think that a government body has possibly told X and TikTok to stop showing my posts on people’s ‘For You’ feeds. This is not organic decline—it is aggressive algorithmic suppression.
This is not just a matter of platform policy. It is a matter of state accountability. If a central body issued this directive to conceal evidence of harm and silence a public interest advocate, it may constitute an illegal act and a breach of democratic protections.
This mass deindexing and algorithmic suppression has concealed my calls for help, suppressed evidence of systemic harm and obstructed public access to testimony that is ethically and legally significant. If this was a coordinated act of censorship, it may constitute a violation of my human rights and a criminal misuse of power by the state.
YouTube Suppression

The situation on YouTube mirrored what I experienced elsewhere, but with the added impact that I paid for promotion.
When I began uploading videos in early October, I received notifications about watch time and reach. I was getting notifications of new subscribers and comments from people prior to the issuance of this shadow ban order.
But since October 26th, I haven’t received any notifications. It seems like YouTube may have muted them. My recent videos have also had very low views even though I have 1.74k subscribers. This suggests YouTube was maybe not showing my videos to my subscribers. This algorithmic throttling is creepy because I could see my subscriber count going up daily, but I had no connection to them because of what seems to be an aggressive shadow ban.
After I published this video on You Tube, my subscription count froze. It had been rising daily. I am wondering if the subscribers are therefore curated as a way to simulate engagement when the Home Office has told them to suppress the reach of my videos. I don’t know as I am in the dark. However, something isnt adding up about this.
Paid Promotion?

YouTube also offered me paid promotion. I accepted promo for five videos around 10th October at £150 each. Google Ads confirmed these promotions. After 26th October, my notifications stopped. A notification subsequently appeared on my account indicating that the promotion had been either paused or halted.
On 17 November, Google Ads sent me an email stating that the promotion from 27th October had been retrospectively disapproved on the grounds of “clickbait” and “sensationalist text”. They did not say this to me at the time that they approved the promotion.
Despite this, Google Ads charged me a further £389 after 27th October, even though they had stopped the promotion.
In total, I paid £579 for promotion that did not deliver reach, leaving me with the sense that the funds went toward suppression rather than expansion. I believe this was not the result of a sudden algorithmic shift or a discretionary change of heart within Google Ads, but rather the implementation of a wider state directive to suppress my reach.
The effect of these actions has left me feeling both isolated and deliberately targeted. What began as an attempt to expand my reach through legitimate promotion ended in silence, with subscribers unable to see my work and funds taken for campaigns that were retrospectively disapproved. The outcome was containment, not expansion, and the isolation it produced is itself evidence of censorship.
What Happened?
This was not coincidental. It signifies, more than likley, that an order from the directive has told a human operator to apply a manual suppresison flag to these videos to protect the bodies involved.
I think that a government body ordered You Tube to stop the promotion. There is no way this sudden change after You Tube had agreed this promotion was user error, or content moderation. This targeted nature of this suppression suggests that this was about political containment.
I am most saddened about YouTube because of the promotion I paid for. Having my reach to subscribers and notifications muted after I have paid £579.00 implies possible monetisation of containment.
Although I am aware that these platforms are following directives from central government, this algorithmic compliance is disastrous. It suggests that social media platforms are now complicit in suppressing a public interest testimony and silencing the voice of a patient desperately seeking help. It is also a violation of my democratic right to speak.
The UK Home Office

A directive of this magnitude, affecting both search engine de-indexing of my content and algorithmic suppression on platforms, can only come from a central body. I am certain that this directive is coming from the UK Home Office.
I think that North Yorkshire police initially triggered the alert to the Home Office. In the month of August 2025, I tagged them in one of my X posts about North Yorkshire County council, (NYCC) not actioning the Public Protection Notice (PPN) that they served on NYCC in April 2025.
It can only be a government body that issued the order for search engines to de-index content so quickly and for platforms to abruptly limit the reach of my content. Additionally, the sudden suppression on TikTok and YouTube took place on October 26 at 8:00 p.m. This is not something a 9–5 office worker could have accomplished. I believe that it was a 24/7 crisis unit that issued this directive.
If I am correct that this state mandated directive is coming from a 24/7 crisis unit, then it is an obscene misuse of power. Crisis units are for monitoring and controlling national security threats, not to silence an advocate seeking help and promoting reform.
On 27th October, I posted on X about this digital siege I was under. I tagged Kier Starmer, asking him to help me. The censorship continued. I had no reply from anyone. This demonstrates that the central government is both aware of and encouraging this censorship. If I am right, then this does constitute state-mandated censorship.
Human Rights Violation

This state mandated censorship is suppressing evidence of documented harm. It is overshadowing my calls for reform, which are in the public interest, and silencing my cries for assistance. I believe that this censorship may constitute the crime of the obstruction of justice and a misuse of state power.
The eclipse of my testimony is also a violation of my human rights. All of my videos and posts safely fall within the remit of protected speech. They do not cite hatred or harassment. My campaign footage is neither defamatory nor slanderous. The language that I use is respectful. It doesn’t dehumanise people or organisations.
Given that my content falls within protected speech, this state mandated censorship and suppression of my online testimony may be a violation of Article 10 of the Human Rights Act.
Article 10 of the Human Rights Act, 1998, includes the freedom to hold opinions and to receive information and ideas without interference from public authority. Suppressing testimony about corporate harm and seeking help is a significant interference with this human right.
This directed suppression of my evidence by the state shows a key defect in a system of working related to freedom of expression and public accountability.
Conclusion

I feel terrified and heartbroken by these events. I am most afraid that the UK government will order a complete closure of my social media accounts. Even though I have issued a statement across all platforms asking them to keep my archive open in the public interest, every time I log in to my accounts, I fear closure.
I am aware that this state mandated censorship is not an attack on me physically but on my online presence, which serves to safeguard the public record. However, I still feel unsafe. I feel the Home Office and the police are watching me. For 30 regulatory bodies to ignore my public pleas for help was torturous enough, but to now silence my voice and cut me off from support is taking it one step too far.
I cannot be sure who is responsible for this suppression of my testimony and for this state-mandated censorship. My belief is that it originates with the Home Office. Whoever is responsible for this, history will hold them accountable. My campaign has been benign. It’s been about calling for help, accountability and healthcare reform. These missions do not warrant this aggressive level of censorship.
I’ve spoken the truth, and I’ve been punished for it. Silenced. It is deeply unjust.

Urgent Update re Digital Censorship as of 25th February, 2026
This is an urgent update to the digital censorship of my campaign as of 25th February, 2026.
X, Twitter
All of my posts have gone from my X feed: Felicia Kate Solomon @myfacialpain. My feed is empty and says @myfacialpain hasn’t posted yet. ‘ Three years of posts have gone from public view. This deletion has happened since I published my blog post on myfacialpain.com on 18th February 2026 about the police surveillance that I’m experiencing from North Yorkshire Police and Police Scotland. My X account has been wiped. I don’t know if my content has been permanently deleted or whether X has held it on their servers, but the ‘@myfacialpain hasn’t posted yet’ is untrue. There were thousands of posts on my X feed that have been deleted. They’ve gone, as I feared.
Additionally, most of the X posts from my X feed that are listed on google lead to a ‘this page does not exist’ sign. All of my content has been wiped.
X was my megaphone. X is where I posted all of my campaign posts to the DHSC and to 40 MPs asking for their help and support. I think that is why a government body has ordered my X feed posts to be deleted: to hide the evidence that so many agencies ignored my suicide risk and pleas for help. Either way, it’s a travesty. Years of posts and thoughtful writing that I raised in the public interest have gone for no reason, other than to protect the agencies involved.
TikTok
Many of my videos have been removed from my TikTok feed: Felicia Kate Solomon @myfacialpain. There is a sign at the top of my feed saying, ‘Some posts are not available due to uncomfortable viewing.’ These deletions include a very neutral introductory video that I posted at the beginning of my campaign, which was just an explanation of what my campaign was. There was nothing uncomfortable about that video, so this appears to be targeted suppression and censorship.
My social media accounts are slowly and progressively now being purged, as I expected, despite me asking all platforms to keep my accounts open. I am unaware whether it is the police, NSOIT, Ofcom or another government body that has told X to wipe my feed and told TikTok to remove some of my videos, but whoever has done this has violated my human right to expression (Article 10.) This was protected speech and I abided by community guidelines at all costs on X and TikTok and was a responsible and kind member of the community.
A Call Out For Help
I have no powers here, but if you are an NGO or a journalist and you see this post, please can you request an FOI to find out who instructed my X account feed to be wiped and why this has happened. Please also see if my content can be reinstated. As I said in my statement, institutional harm is everyone’s business, and I was campaigning for an end to systemic neglect. Now with an empty X feed with no posts, reformers cannot find my work. Please speak on my behalf to ensure this doesn’t go unnoticed.
This is a violent infringement of my human rights to free speech. To then be stalked and surveilled by police following this digital erasure is state overreach at its very worst. It defies cruelty. I haven’t deserved any of this. My campaign was a patient asking for help and trying to help ensure others don’t endure what I have. I do not deserve to have my voice erased in this way.
Video 19: Advocacy Video Campaign
In this video, I had not become aware about the algorithmic suppression on platforms. This video mainly speaks about the de indexing from search engines. My awareness about the algorithmic suppression came days later. Thank you.
Photo Credits: Sora Shimazaki, RDNE, Marco Bianchetti and This is Engineering and Goumbik on Pexels. Gama Films on Unsplash.

2025-11-22 08:33
On The Digital Suppression of My Campaign: Stage One.
Disclaimer: The Digital Suppression of my Campaign is not an attack on individuals or institutions. It is raising awareness about the dangerous reality of data suppression online, digital rights and concealment of public interest testimony. This post documents my lived experience, which raises serious concerns about transparency and the rights of whistleblowers to speak freely under Article 10 of the Human Rights Act.
Trigger Warning: This blog post references suicide and mental health neglect that some readers may find distressing. If you are affected by these topics and need support, please call NHS 111 (option 2) or the Samaritans freephone on 116 123.
Summary

This blog post and video document the early stages of the digital suppression of my campaign by either the NHS or central government bodies. It discusses the impact this has had on my online visibility, including the suppression of my calls for assistance, the obscuring of a public interest testimony, and the concealment of documented evidence of statewide corporate harm.
This post and the campaign video summarise the purpose of my campaign. It requests that all platforms (X, TikTok, Vimeo, and YouTube) keep my archives and accounts open in the public interest in the event that the UK government requests the closure of my social media accounts.
The Professional Standards Authority

A large part of my campaign has been my silent diaries. After I published my campaign videos across social media platforms, I have been publicly documenting every day of silence from regulators and MPs. This video concludes 44 days of regulatory silence, as my campaign ended on Friday, October 31st, 2025, due to what I believe to be censorship and digital suppression by government bodies.
I have heard from the Professional Standards Authority (PSA). The PSA contacted me on X, (formerly Twitter) to say that they cannot intervene in personal cases. They said they were “sorry” for my experiences and distress, and they sent me a link to Samaritans to assist with my distress. They explained that they are the regulators of regulatory bodies and encouraged me to provide feedback.
My Reply to the PSA

I thank the PSA for contacting me. I understand it is out of their jurisdiction to help me personally because the PSA’s role is to oversee regulatory bodies, not to assist individuals. However, I found the link to the Samaritans that they sent me insulting, as it communicated an act of deflection on their behalf. Samaritans cannot help with twelve years of statewide institutional harm.
Even though the PSA cannot help me personally, they still have a role to play in the bigger picture of my case. My story is one of statewide systemic neglect. The neglect extends across 19 NHS trusts, two local authorities and a GP practice. My story points to a systemic flaw or defect in the system’s inability to catch this harm.
The fact that every bit of this harm has gone unregulated indicates a breakdown in the functioning of our system’s defences: a cog that is not working correctly.
A Call For Review

I urge the PSA to use cases like mine for parliamentary review and scrutiny so that this harm does not occur to other patients. In order to avoid harming other patients in the same way, we must have a non-aggressive and non-blaming discussion about widespread neglect and what we can do to stop it in the future. We need a paradigm shift and an end to the “lessons have been learnt” culture. It’s time we stop accepting these platitutudes. It’s time that patients get real redress and accountability when things go wrong in healthcare.
Additionally, as the overseers of regulatory bodies, it is their business to address these 44 days of silence from regulators. The lack of response from regulatory bodies shows that they have turned a blind eye to a suicidal patient calling for help. It also shows that they have ignored serious patient safety concerns that I have raised. By ignoring my concerns, they are not protecting the public, which is what their role is. It is thus the PSA’s responsibility to address the silence of the bodies it regulates if regulation is truly about protecting the public.
Digital Suppression of My Campaign

My awareness about the digital suppression of my campaign has come in stages. This video documents my first stage of awareness. I became aware in mid October, 2025 that numerous links to my X posts had disappeared from Google. There were very few if any links to my X posts under my name that included my name and NHS trusts. The only links are to generic posts from many years ago.
I became aware that NHS trusts or a central body were likely submitting ‘Right to Be Forgotten Requests’ (RTBF) to Google to remove links from my X posts on Google. NHS trusts most likely submitted these requests to Google based on false allegations of harassment, defamation, or data breaches. If they are doing this, these grounds don’t qualify. All of my social media posts and vidoes fall within protected speech of Article 10 of the Human Rights Act, (Freedom of Expression.) They do not contain misinformation. Nor do they promote hatred or discrimination and they contain no defamatory or slanderous content.
As part of this first stage of this digital suppression of my content, I’ve also observed a sign under my X profile on Bing and Yahoo saying that they are disallowed from crawling my site. This is a high-level block that only a governing central body could have potantially made.
Screenshot of my X profile on Yahoo, which says, ‘we cannot show you a description of this page.’ Bing is blocked from crawling my X profile.
Impact on Me
Whatever grounds the NHS trusts have for making these RTBF requests to Google, the removal of these links has significantly decreased the visibility of my campaign content.
This action means that my urgent calls for help are now less visible in the public domain. My public interest-driven demands for NHS reform and transparency are muted, and my documented evidence of corporate harm has been suppressed.
If NHS trusts or central bodies are submitting RTBF Requests to Google, they are doing this to protect their reputation and to keep this story out of the public record. However, they are suppressing the voice of a vulnerable patient who is desperately seeking help. This digital suppression is also reducing the visibility of a public interest disclosure. These actions could constitute the obstructing the course of justice.
My Campaign Mission

In light of this digital suppression of my campaign, I am naturally concerned that the NHS or regulators will request the closure of all of my social media accounts. I fear they will do this to conceal my documented evidence of harm throughout the NHS. As a result, I am summarising my campaign as part of my request to all platforms to keep my archive and accounts open in the public interest.
Felicias Campaign has been about obtaining an urgent independent review of my medical condition and implementing immediate mental health support to assist me while I am in crisis. This has not been successful. Despite making four public pleas for help to Penny Dash, the DHSC, 30 regulatory bodies or 40 MP’s, I have received no response.
I have also been campaigning for an end to systemic neglect so that no one endures what I have suffered. I have been campaigning for greater accountability and transparency within the NHS so that patients get real redress for their grievances. Lastly, my campaign has been about calling for urgent patient safety reform and improved crisis care across the NHS network.
All of these missions are in the public interest. They are to promote a more transparent healthcare system that protects patients. Patient safety and institutional harm are everybody’s business. I am therefore asking all platforms to keep my archive open in the public interest. This will enable reformers to find my work now and in the future.
No Defamation or Slander

All of my campaign videos and posts were carefully and responsibly created. The mental health videos and silent diaries include integrated trigger warnings. The trigger warnings that I include ensure safe viewing, and the footage is intended to end mental health neglect, not to promote self-harm.
My footage’s tone is neither defamatory nor slanderous. I have not named any clinicians or spoken negatively about any clinicians or institutions. I have redacted all clinician names from the medical documents that I have uploaded. There are no physical descriptions that could be used to identify anyone.
My campaign has been factual and evidence-based. All of the medical documents that I have uploaded are mine. They are from my medical records and they pertain to me and my medical history. As a result, I have not violated any data protection laws by using them. They have been used to seek assistance, particularly with regard to my scans, and to flag serious patient safety incidents.
My tone has been respectful throughout. My intention has not been to bring disrepute to the NHS. It has been about seeking help and accountability for what has happened to me. These are very different intentions.
Closing Comment

I will be documenting the far more aggressive digital suppression of my campaign that happened towards the end of October, in my next post. This involves major algorithmic suppression and throttling across social media platforms and further de inexing of my campaign content online.
I feel threatened and targeted by this digital suppression. I have told the truth in a responsible manner, and government bodies are now punishing me for it Because all of my requests for help have gone unanswered, I also feel powerless in this circumstance.
Due to this digital suppression, I ended my advocacy campaign on Friday, October 31, 2025.
Setting The Record Straight

As a closing comment to this post, I would like to say this. I will do everything in my power to save my life. I wholeheartedly believe in the preservation of life, and I deserve to live in spite of this corrupt oppression. Truly, I will do my best. However, if I am unable to hold on, I would like to make it clear:
If I don’t make it, it’s not mental illness. I do not have a mental illness. I am in a life-threatening crisis because of physical pain and institutional harm. There’s a difference. It will not be because of weakness or cowardice. I am not weak. Nor will it be an act of defiance.
It will be the culmination of twelve years of institutional harm, complicity, regulatory silence, and institutional censorship and silencing.
It is critical that people understand this. If I am unable to survive, I don’t want their corruption and complicity to be diagnosed as my instability. That would cost me my integrity, and I don’t want that.
The weight of this oppression is too heavy. Nobody can be expected to carry this. No one. I’m not superhuman.
I ask that this be heard and understood with the reverence and respect it merits.
Thank you so much.
Video 18: Advocacy Video Campaign
Photo Credits: Pavel Danilyuk, Brett Sayles, Tdcat, Markus Spiske, Muffin and Lara Jameson on Pexels. Alora Griffiths on Unsplash.

2025-11-10 11:30
On Institutional Silence and State Coerced Cruelty
Disclaimer: On Institutional Silence and State-Coerced Cruelty is not an attack on individuals or institutions. This blog post highlights the serious issue of institutional science in the public interest to help move towards a healthcare system with more accountability.
Trigger Warning: This blog post and accompanying video contain sensitive content relating to mental health neglect, suicide and fears of posthumous gaslighting. Please watch the video with care. There is a long list of helplines provided at the end of the video should you need support.
In the meantime, if you need support, please call NHS 111 (option 2) or Samaritans freephone on 116 123.
Summary

In my previous post and campaign video, I documented that I have made three public requests on X to Penny Dash (chair of NHS England), the Department of Health and Social Care (DHSC), 30 regulators, and 40 elected representatives, asking them to arrange an independent review of my medical condition and to implement urgent mental health support for me.
I have not had a response from any of them. Thirty regulators and 40 MPs have met me with a wall of silence.
This blog post and video document how this systemic cruelty and coldness feel. It also revisits my story, which I have framed as an institutional cover-up. Lastly, it expresses my fears that in the event I don’t survive this, the state will posthumously gaslight me and rewrite my story.
Coldness

I don’t think I can find the words to express how this coldness and silence from the state feel. Thirty regulators and 40 MPs constitute the state.
I have made a rational and reasonable request to all of them. I have requested an independent review of my facial pain condition free from institutional deception and cover-up. This request is based on the fact that the majority of NHS trusts I have visited have identified abnormal pathology in my case. However, they have not acted on these abnormal findings. It is therefore a fair and reasonable request that clinicians explain to me what these abnormalities are and use these findings to inform an accurate diagnosis of my condition.
A major part of my campaign (#FeliciasCampaign) has been my request for regulators to put in place urgent mental health support for me. I have been clear to NHS England and the DHSC that I do not feel I will be able to survive without immediate mental health support. My request is also reasonable given that Tees, Esk and Wear Valleys Trust (TEWV) and North Yorkshire County Council have left me with no support or safeguarding after I survived a fatal suicide attempt in February 2025.
Institutional Silence

For all of these bodies to respond to me with silence defies the definition of cruelty. This institutional silence from regulators and MPs is calculated coldness. This isn’t an administrative oversight. They are choosing to ignore my pleas for help because reaching out to me would mean acknowledging fault. Regulators are choosing to protect the institutional image of the NHS trusts and GPs involved in my case. They are putting reputational protection over the cost of a human life.
Their silence demonstrates a profound disregard for my well-being and the sanctity of my life. It’s despicable.
Institutional Cover-Up

This institutional silence from regulators and MPs seems to prove what I have been saying all along: that my story is an institutional cover-up. I believe that it is.
It started with my medical problem. It began with denial that my problem was an infection in 2014 at Leeds Teaching Hospitals. An ophthalmologist kicked me off the ward and stopped all of my antibiotic medication. The covering moved onto Guy’s and St Thomas’ NHS Foundation Trust, where I believe the dental radiologist who performed the last sialendoscopy in January 2017 was not honest about the clinical findings.
Then the covering and denial went through to The North Manchester General Hospital, who, in spite of finding abnormal pathology in my parotid tissue, refused to culture it or do further diagnotis tests on my tissue. Following this, I believe that it is possible that Charing Cross Hospital have deleted or concealed some of my radiology images from an MRI neck scan that they performed on 23rd May, 2019. I believe that this hospital may have concealed this evidence to cover for the salivary gland unit at Guy’s Hospital.
Lancashire Teaching Hospitals, Aintree Hospital, and the Manchester Royal Infirmary subsequently shirked their responsibilities. Chorley and Preston Hospital referred me to Manchester University NHS Trust. Aintree University Hospital refused to see me for no reason, and the Manchester Road Infirmary directed me back to Guy’s Hospital instead of taking action internally.
I then experienced obscene discrimination and denial of care at NHS Fife and NHS Lothian, where they too ignored abnormal clinical findings. I then experienced severe gaslighting at South Tees. Two clinicians refused to acknowledge my problem, and then York Hospital found an abnormality on an MRI neck scan in July 2022, which they failed to act on.
Mental Health and Social Services


This widespread abandonment and harm isn’t confined to medical teams. It has spread to mental health services and adult social care. I believe that both of these agencies are complicit in the covering up of the situation. Tees, Esk and Wear Valleys Trust (TEWV) has denied me crisis care and mental health support following my suicide attempt. North Yorkshire County Council (NYCC) has then ignored three safeguarding concerns. They also terminated my statutory support in 2023 for no reason.
Additionally, both of these organisations have been responsible, I believe, for trying to cover up the scale of my crisis. This is illustrated by TEWV’s crisis team telling NYCC to close down the safeguarding concern that the CQC raised in February 2025, which NYCC did. They did not action the safeguarding concern, leaving me at risk.
GP

Last but not least, my GP surgery, Ampleforth Surgery, has been falsifying my records to conceal my suicide risk and downplay the extent of my mental health crisis.
Conclusively, I believe that all of the above prove that my story is an institutional cover-up. I believe that the institutional silence from regulators and MPs is protecting this cover-up. Their silence has made regulators now complicit in the harm.
Fears of Posthumous Gaslighting

This video also documents my fears about posthumous gaslighting. If my story ends tragically, and I do not survive, I am afraid that the state will conceal the facts. I fear that the truth will never be revealed.
I have no control over this. However, I am determined to reveal two aspects of this cover-up: the potential removal of files from Charing Cross Hospital and the falsification of my medical records by Ampleforth Surgery. These are the two most significant injustices in my story that have caused me the most harm.
I have made two public requests to the ICO on X to carry out an audit trail of my records regarding these incidents. However, on both occasions they deflected responsibility and ignored me. It is in the public interest for the ICO to investigate both of these incidents. This misconduct does not only undermine my safety, but it also compromises the integrity of our entire healthcare system.
I also state in this video that it is in the public interest for regulators to investigate the leadership at Ampleforth Surgery. There was a serious incident at this practice in August 2023. A man set fire to the surgery, for which I am very sorry. It was a terrible tragedy. Thankfully, no one was hurt.
However, the facts never came to light about why he did it. The fire, coupled with my disclosures, indicates a possible lack of integrity at this practice. Regulatory bodies must investigate this practice to ensure the safety of other patients.
Conclusion

The institutional silence from regulators proves a contradiction to everything that they say they are about. Regulators exist for the sake of the public. They exist to protect the public. Ignoring a patient in crisis and multiple serious patient safety incidents that I have reported throughout my campaign does not protect the public. It allows misconduct to go unregulated. It also allows it to continue
If regulators do not adhere to their own guidelines, follow the duty of candour and investigate complaints with rigour, we will be forever stuck in a ‘lessons have been learnt’ culture. Patients will never receive redress for their complaints and critical oversights, and a lack of accountability will continue to harm patients across the NHS system.
This institutional silence and state-enforced cruelty are unacceptable.
Video 17: Advocacy Video Campaign
Photo Credits: Mick Haupt, Simon Lee and Scott Umstattd on Unsplash. Olly, Ivan S and Mikhail Nilov on Pexels.

2025-11-10 11:10
Institutional Abandonment: DHSC Ignores my Plea for MH Support
Disclaimer: ‘Institutional Abandonment: DHSC Ignores my Plea for MH Support’ is not an attack on individuals or institutions. It is an urgent request for assistance in sustaining my life, as well as a call to end mental health neglect. I am raising this issue in the public interest to ensure that we see an improvement in crisis care across the UK.
Trigger Warning: This post discusses suicide and mental health neglect that some readers may find distressing. If you require assistance, please call NHS 111 (option 2) or the Samaritans freephone number 116 123.
Summary

My recent blog posts document how, following my surviving a fatal suicide attempt in February 2025, mental health services and social services have left me without any support, outreach, or safeguarding. It’s damning.
There is no one to turn to, and every day presents a challenge to persevere. The pain of this institutional abandonment hurts like no other. TEWV and North Yorkshire County Council’s abandonment has added another layer to the years of institutional harm that I have experienced. This post documents my direct appeal to NHS England and the Department of Health and Social Care (DHSC) for their intervention and help.
The Pain of Institutional Abandonment
![]()
I created the video below as part of my campaign video advocacy series. In this video, I speak directly to TEWV and NYCC, telling them how their silence and abandonment feel. I explain that if I don’t survive, it isn’t because I haven’t ‘engaged’ or am ‘complex’. These narratives are frequently used against patients who die as a result of mental health neglect.
I make it clear, especially to Tees, Esk and Wear Valleys Trust (TEWV,) that I have made numerous attempts to engage, but they are the ones who have discharged me and barred me from attending Accident and Emergency at Scarborough Hospital for mental health support. They have cut off all crisis care and refused to help me. It is not me. While I will do everything I can to stay alive, if I do not, I do not want their failure and neglect to be interpreted as my refusal to engage.
My Plea to Penny Dash

I am profoundly struggling. In this video, I make a request to Penny Dash, the newly appointed chair of NHS England, and to the Department for Health and Social Care for them to put some urgent mental health support in place for me. I made this public request in August 2025 and again in September 2025. I have made it abundantly clear that I do not think I will survive without help.
In this video, I ask them to break their silence, and I articulate how institutional silence feels. I ask Penny Dash why the NHS is treating me in this cruel manner. I ask her why the NHS has frozen me out in this way.
In this video, I ask Penny Dash to put my safety first. I remind her that she started her tenure as chair of NHS England speaking about the importance of patient safety and transparency. In only July and August 2025, Penny Dash spoke about the importance of holding individual teams and boards to account, and she proposed the streamlining of safety regulation.
I plead with Penny Dash and the Department of Health and Social Care (DHSC) for them to put in place some urgent mental health support to ensure that my life does not end in tragedy.
Conclusion

I posted this video on X and tagged in NHS England, the DHSC and 30 other regulatory bodies. I also copied in forty elected representatives, including Baroness Hollins. Baroness Hollins has written extensively on safeguarding failures and mental health abuse. This video was shared with them all twice, but I have received no response.
I’ve been met with more silence.
This lack of response from them is not an administrative oversight. It is a calculated choice to ignore my urgent pleas for help. Their silence highlights the sinister contradiction between what these governing bodies preach and what they actually do. They are choosing to put institutional convenience over saving my life. By choosing to remain silent, they are now complicit in the harm.
This silence is not patient safety or institutional accountability. Their refusal to respond to my request for assistance puts the patient in danger. It constitutes institutional cowardice and state-coerced cruelty.
The lack of response from NHS England proves that patient safety is not currently a reality that they embody in their practice. It is a politically correct slogan that they flout for convenience.

Video 16: Video Advocacy Campaign
Photo Credits: Mart Production, Nejc Kosip and Germar Demon on Pexels.

2025-11-10 10:58
My Statement To The Medical Fraternity and A Call for Reform
Disclaimer: My statement to the medical fraternity is not an attack on individual clinicians or institutions. It is calling for a compassionate end to my situation. This post is also calling for healthcare reform.
Trigger Warning: This post discusses the topic of assisted suicide that some readers may find distressing. If you require assistance, please call NHS 111 (option 2) or Samaritans freephone number 116 123.
Summary

This blog has documented with forensic precision the unbearable physical pain I have now been in for 12 years. It also documents the repeated obstacles that I have faced within the UK healthcare system in trying to get a diagnosis or medical treatment for my facial pain condition. Despite exhaustive efforts, I have been met with deflection, gaslighting and a covering of evidence by 19 NHS trusts.
I’ve also documented how this trauma has led to a cataclysmic mental health crisis for which I have no support or help. It has led to an attempt to end my life in February 2025, after which mental health services, (TEWV) and social services (NYCC) denied me support or safeguarding.
This post and video document my statement to the medical fraternity. It requests either a compassionate end to my situation with the medical treatment that I need to get me out of this pain or a report that will end my story in peace. It also calls out to our health minister, Wes Streeting, to implement urgent healthcare reform so that patient safety becomes a reality for patients, not just a political slogan that politicians flout for convenience.
Dignitas Application

I cannot control the choices that the medical fraternity are making in response to my situation. I cannot stop them from gaslighting me and ignoring abnormal pathology, and I cannot make them treat my condition. None of these, do I have any control over. The only control I have is over my own decisions and actions.
I cannot live with this pain any longer. It has got progressively worse in recent years, especially around the left side of my head. It feels like someone is screwing a corkscrew into the top of my head. The pain in my parotid area is worsening as is my periocular pain. I am in agony.
My Request For Dignity

In 2021, I decided that I wanted to walk away, both from the pain I am in and this impasse with the medical fraternity, but I wanted to walk away in peace. I wanted to walk away with my dignity intact and in a way that restores the foundations of my value system: kindness to the soul and to the body. It would be harmful to me if I took my own life. I do not want this.
In 2021, I made a formal request for Dignitas to prepare an accompanied suicide for me. I made a formal request to Dignitas for an accompanied suicide, citing my experience of unbearable and uncontrollable pain as the basis for this decision.
An assisted suicide would enable me to walk away from the pain and from this toxic battle in peace. I would be able to end my life and the pain with support and compassion. I would not be alone, and I would not suffer. This is what I wish for if they are unable to alleviate this pain.
The Required Report

In order to meet the legal pre requisites for an accompanied suicide and in order for Dignitas to process my application, they require a medical report from a clinician proving that my pain is not controllable. Dignitas asks that a clinician write a report to confirm that I am receiving state-of-the-art treatment and that medics have exhausted every resource to get me out of this pain.
Additionally, I have had to declare in my biography summary to Dignitas that I have been in a life-threatening crisis for six years due to this pain that I am in. Dignitas also requires a psychiatrist to write a report certifying that I am of sound mind to make the decision to end my life. Dignitas cannot process my request for accompanied suicide without these reports.
I Cannot Get The Report

I have asked six clinicians across the UK to provide this report for me, and that includes three TEWV psychiatrists. They have all said no. Thus, my application for an accompanied suicide is ‘pending’. Dignitas cannot process my application without these legal papers.
My Statement

This post and this campaign video serve as my statement to the medical fraternity to say the following: You can’t have it both ways. You can’t ignore me like this and ignore my medical condition when you know there is something clinically wrong and expect me to live with this pain forever. You know there is something wrong. Most of the NHS trusts where I have been have found abnormal pathology, so you know that I have a clinical problem. You know I am not making this pain up.
If the clinicians I’ve seen hadn’t discovered any abnormal pathology, I’d understand you not acting, but that is not the case. You found:
- Infection markers have been consistently elevated.
- A left levator that has collapsed.
- Glandular malfunction.
- Parenchymal damage to my left parotid gland.
- There are reactive lymph nodes.
- Abnormal enlargement of the left masseter.
- An unexplained abnormality in my left buccal fat pad and pterygoid muscle.
- Unexplained visible abnormalities in my NHS Lothian and York Hospital scans. The radiology images in question show an enlarged left frontal lobe, nasalis damage and orbital bone damage.
All of these findings point to chronic infection or inflammation as being the likely cause of my pain. Based on these findings, your decision to not act is not acceptable.
My statement to the medical fraternity is this: if you will not act on these clinical findings and relieve me of this pain, then I am asking that you provide me with this report that Dignitas requires to process my application for an assisted suicide so that I can walk away from this pain in peace. It’s only fair.
A Call for Healthcare Reform

My story raises serious patient safety concerns. I have highlighted in this blog and in my videos a series of serious patient safety incidents. These incidents include:
- Ignoring and failing to take action on abnormal scans.
- NHS trusts deflecting responsibility.
- Dangerous Gaslighting.
- Prematurely discharging me from care.
- Leaving me with no mental health support after a suicide attempt.
- Returning lethal substances to me after a suicide attempt.
- Denying me safeguarding when I am high risk.
- The falsification of my medical records.
All of these have put me at risk. They have delayed my diagnostic outcome and prolonged my suffering unnecessarily. However, this isn’t just my story. This is potentially every patient’s story, and a failure by regulators to address these concerns compromises not just my safety but the safety of all patients across the NHS network.
To Wes Streeting
I am calling on Wes Streeting to implement urgent reform so that patient safety becomes a reality for patients in the UK, not just a politically correct slogan that is used by politicians for convenience.
These proposals for reform include:
- Protecting NHS whistleblowers so that they are safe to flag patient safety concerns without job loss or retribution.
- Combating discrimination and stigmatisation in healthcare. Equal access to healthcare for everyone.
- Robust regulation of management. Hold management accountable.
- Learning to say sorry and put things right. Remembering that saying sorry does not make doctors liable for legal action.
- Putting patient safety at the top of the healthcare agenda so genuine patient care supersedes clinicians and hospitals covering up failings to protect their institutional image and the reputation of their colleagues.
Conclusion

My statement to the medical fraternity is an urgent call out for an end to my suffering. Twelve years is enough torture. This video also calls for healthcare reform. A story like mine is also a critical reminder about the urgent need to make patient safety the top of the healthcare agenda and to increase regulation of managers to ensure that the professional duty of Candour is adhered to in healthcare settings.
It is also a stern reminder of the dangers of delayed diagnosis and the culture of silence.
It is time for real change: an end to the cover-up culture and the “lessons learnt” culture. A new landscape must emerge to allow for patients to get true accountability and redress for their complaints.
Video 14: Advocacy Video Campaign
Photo Credits: Towfiqu Barbhuiya, David Lowe and Alexander Grey on Unsplash. Gelgas, Pixabay, MasterCowley, Karola G and Pavel Danilyuk on Pexels.

2025-10-29 09:26
North Yorkshire County Council: Disregards Police PPN
Disclaimer: North Yorkshire County Council: Disregards Police PPN is not an attack on individual social workers or institutions. It is highlighting critical failings in social care in the public interest. I do not want other vulnerable adults to ensure what I have suffered.
Trigger Warning: This post makes reference to suicide and safeguarding failures that some readers may find distressing. If you need support, please call NHS 111 (option 2) or freephone Samaritans: 116 123.
Summary
My previous blog post highlighted how North Yorkshire County Council, (NYCC) stopped my statutory support in 2023 without warning or reason and went against GP and psychiatry advice. It also documented how they ignored a safeguarding concern raised by the Care Quality Commission in February 2025.
This post highlights how two months after failing to action a safeguarding concern by the Care Quality Commission, North Yorkshire County Council then disregarded a Public Protection Notice, a PPN issued by North Yorkshire police in April 2025—just two months after surviving a suicide attempt. The PPN was served on NYCC to safeguard me and provide me with support.
What Happened?

Two months after surviving a suicide attempt and two months after North Yorkshire County Council ignored a safeguarding concern raised by the CQC, an incident occurred at my home.
Two neighbours fly-tipped my garden. They left mounds of garden waste, road signs and bracken in my garden. They also ripped off my entry gate and threw it onto a mound of bracken.When I confronted them about it, the husband of the couple was aggressive and abusive towards me. He verbally abused me, and I felt extremely threatened and frightened.

I complained to my landlord, Yorkshire Housing, who did not reply to my complaint. I complained to the fly-tipping unit at North Yorkshire Council, who said it was the ‘landlord’s responsibility’ to deal with it and deflected back to them.
Following this, I contacted the adult social care team at North Yorkshire Council. I explained how threatened I felt by my neighbours. I am pleased with them reconsidering the safeguarding request by the CQC. They refused. They told me once again, ‘You know how to complain.’ I explained that my landlord, Yorkshire Housing, had not replied to my complaint, but they still refused to help.
My neighbours then retaliated and put in a false complaint to Yorkshire Housing about me ‘leaving out rubbish’, which was untrue. This led to Yorkshire Housing sending me a threatening email, titled ‘ASB Breach’. The content of the email said I was under investigation for an anti-social behaviour violation regarding leaving out rubbish.
Then I felt really threatened. I didn’t just have my neighbours harassing me. I had my landlord making allegations about me based on lies. For the second time, I pleaded with North Yorkshire County Council. I asked them to put in place safeguarding, but they said, ‘No, sort it out yourself.’
Public Protection Notice, (PPN)
I called the police because I felt unsafe and under threat. On 5th April 2025, a lovely police officer from North Yorkshire Police visited me at home. The local constabulary knew about my recent suicide attempt, as they had carried out a forced welfare check on my property in February 2025. The police officer took a video recording of my bins, which were immaculate.
She asked me why TEWV was giving me no support, but I told her they had discharged me from their care. I told her that North Yorkshire County Council had continually withdrawn my support and kept closing my file in spite of safeguarding concerns being raised about me.
On 5th April 2025, the police served a Public Protection Notice a PPN on NYCC to give me support and safeguarding. A Public Protection Notice is a record of a safeguarding concern to inform a multi-agency response.
I heard nothing from North Yorkshire Council. Just like the CQC safeguarding concern they ignored from February 2025, they disregarded the PPN it and took no action.
Conclusion

This is the third safeguarding concern raised about me that North Yorkshire County Council has ignored and failed to take action on. These breaches violate the Care Act, 2014, and possibly the The Anti-Social Behaviour, Crime and Policing Act, 2014 and they are putting me at significant risk.
This is unacceptable conduct. Local authorities must be held to account for these actions.
I am calling on North Yorkshire County Council to publicly account for these failures, and I am calling on the Care Quality Commission and the Local Government Ombudsman to investigate these serious breaches in duty of care. Vulnerable adults must be protected.
Video 14: Advocacy Video Campaign
Photo Credits: Keira Burton, Safi Erneste and Mart Production on Pexels.
2025-10-28 09:54
North Yorkshire County Council: Safeguarding Failures and Neglect
Disclaimer: North Yorkshire County Council: Safeguarding failures and neglect is not an attack against any individuals or institutions. This post is exposing safeguarding failures which I am raising in the public interest to prevent this neglect from happening to others.
Trigger Warning: This post makes reference to a suicide attempt that some readers may find distressing. If you need support, please call NHS 111 (option 2) of Samaritans freephone: 116 123.
Summary

The systemic neglect that I have documented in this blog extends beyond medical teams and mental health services. It has extended to social services.
In the past three years, North Yorkshire County Council (NYCC) has neglected to address safeguarding concerns that have been raised regarding me and has withdrawn statutory support, thereby exposing me to risk and vulnerability.
Withdrawal of Statutory Support

In March 2022, North Yorkshire County Council, adult social care, assessed me as meeting the criteria for statutory support. They agreed to put in place direct payments, which is a pathway of support I had received with my previous authority, Calderdale Council. While awaiting the implementation of that support, NYCC arranged for a Support, Time, and Recovery (STR) worker to assist me.
This was a lifeline for me at a time when I was experiencing bullying and gaslighting at South Tees NHS and York Hospital. My STR visited me at home weekly. However, in 2023, a new social worker took over my case. She turned up at my house and announced she was stopping all of my support.
The social worker did not reassess me, which is why this withdrawal of my support felt so unfair. She did not discuss the reasons with me or include me in any of her decisions. She also went against GP and psychiatric liaison guidance. Both my GP and psychiatric liaison services from Scarborough A&E wrote to North Yorkshire County Council and explained that a withdrawal of my support would put my mental health at risk.
They ignored this recommendation and terminated all support.
Ignored Complaints

I complained to North Yorkshire County Council three times about them withdrawing my support without warning or without reassessing me. In my complaint, I asked the council to give me reasons regarding the cessation of my support, but they did not reply. I included numerous local councillors and Members of Parliament in my complaint. However, none of them replied to me.
I did receive an email from the mental health lead at NYCC. She said that they would try and put support in place. However, a different social worker came to see me and just confirmed they were closing my file. That didn’t constitute a reply. It was compounded abandonment.
Refused Referrals

In 2023, North Yorkshire police referred me back to North Yorkshire County Council for safeguarding and support. However, NYCC sent a worker from their non-statutory Living Well scheme to see me at home three times. They then closed my file again. This was a refused referral. The referral from the police requested that safeguarding and statutory support be implemented; however, neither was provided.
My file remained closed.
Safeguarding Failure

In January 2022, the General Medical Council’s Victim Support Service sent a safeguarding concern to North Yorkshire County Council about my suicide risk. Despite implementing an STR in 2023, they failed to address the safeguarding concern. They put no safeguarding in place.
In February 2025, after I survived a fatal suicide attempt, their regulator, the Care Quality Commission (CQC), asked NYCC to safeguard me from TEWV (Tees, Esk and Wear Valleys NHS Trust) and my GP, Ampleforth Surgery.
However, they took no action and closed down the safeguarding concern. On 6th March 2025, a social worker told me that they were closing down the safeguarding concern because ‘I knew how to complain’, and I knew ‘how to ask for help’.
Breaches of the Law

Many of these failures violate obligations under the 2014 Care Act. However, the law aside, safeguarding concerns are dangerous, and ignoring them puts vulnerable people at risk of harm. The potential breaches of the law by NYCC include:
By not replying to my complaint in 2023, NYCC breached The Local Authority Social Services and National Health Service Complaints (England) Regulations 2009.
By not giving me warning or a reason why they stopped my support, NYCC breached The Care Act 2014, Article 9, which states that local authorities must work in partnership with service users and inform them about any decisions regarding their care.
Ignoring safeguarding concerns after a suicide attempt, and when raised by the CQC may be a breach of safeguarding laws and regulations.
Local authorities have a duty to investigate and protect vulnerable individuals under the Care Act 2014 and the Children Act 1989. Failure to act is unacceptable.
Regulation 13 of the Health and Social Care Act 2008 requires healthcare providers and local authorities to safeguard service users from abuse and improper treatment. Ignoring concerns breaches this duty.
Conclusion

North Yorkshire County Council’s actions have been the main reason I have sunk to this very dangerous predicament. The removal of my support and the refusal to safeguard me has left me vulnerable and open to risk. It’s been institutional abandonment. They have neglected their duty of care towards me.
To be left with no support or safeguarding at a time when I have been this in need of help has left me isolated and afraid. It has left me to deal with the instituitional bullying from these numerous NHS trusts alone.
I am calling on North Yorkshire County Council to publicly account for these failures, and I am calling on the Care Quality Commission and the Local Government Ombudsman to investigate these serious breaches in duty of care. This is not just my story. It’s about ensuring the protection of vulnerable adults across the social care network.
Video 13: Advocacy Video Campaign
Photo Credits: Mateus Souza, Cottonbro Studio, Ann H, Pavel Danilyuk, Ron Lach and Kampus Production on Pexels.

2025-10-26 04:45
My GP Practice Falsifying My Medical Records: Ampleforth Surgery
Disclaimer: My GP Practice Falsifying my Records is not a personal attack on individual clinicians or institutions. It exposes serious breaches of data protection law and patient safety principles. I am raising these incidents in the public interest to promote urgent patient safety reform so that future patients are protected from such harm.
I also wish to clarify that these medical records belong to me. All clinicians names have been redacted. I am therefore not breaching Data Protection Laws by uploading them as evidence onto this post.
Trigger Warning: This post contains content relating to suicide and medical record falsification that some readers may find distressing. If you are in crisis and need support, please call NHS 111 (option 2) or Samaritans’ free phone 116 123.
Summary

Over the last two years, my GP practice, Ampleforth Surgery, has falsified and retrospectively amended my medical records on nine occasions. They have done this to conceal my suicide risk and to cover for an abnormal MRI neck scan that they and York Hospital did not action in July 2022. These incidents include:
Deleting Records

On May 17, 2024, I went to the Scarborough Accident and Emergency department for help with suicidal feelings. The secretary at the practice entered my attendance onto my record as ‘Seen at Accident and Emergency, suicidal feelings, ongoing episode.’
Three weeks later, that record disappeared. One of the leading GPs deleted that record. There is nothing ony records showing that I attended A&E for suicidal feelings on 17th May, 2024.

Discharge summary from Scarbrough A&E showing I attended on 17th May for help with suicidal feelings.

Medical records showing no record of me attending A&E for suicidal feelings on 17th May, 2024.
I believe that my GP pracice did this to cover for TEWV (Tees, Esk and Wear Valleys NHS Trust), who had wrongly discharged me from their care, and to cover for themselves for providing me with no support. They did this to conceal my suicide risk.
When on 3rd July 2024 I spoke out on social media, (X) about this deletion, my GP practice added an ‘admin note’ to the record. I believe this action was to backtrack and cover for the deletion.

Medical record, which shows how the practice added an admin note about this deletion, the day I spoke out on X about this.
Falsifying Records

Incident 1: One of the leading GPs at Ampleforth surgery has falsified my records. She has indicated that she did two depression reviews with me that never occurred. I have no idea who she is because I have never met or spoken to her. She made the following recording:
On March 29th, 2023, I attended the Scarborough A&E department for help with suicidal feelings. The GP entered that she did two depression reviews with me either side of this visit. She falsely recorded that she did a depression review with me on March 23rd, 2023, and March 31st, 2023. These reviews did not happen.

These is the record of one of the false depression reviews that the GP recorded that never happened.

This is the other record of one the false depression reviews that the GP recorded that never happened.
I believe the GP did this to make it appear that Ampleforth surgery was giving me support when it wasn’t.
Incident 2

Incident 2: In June 2024, I developed a rash on my right arm. I emailed the practice, and I requested some cream for the rash. I included seven clear photographs of my rash with the email. My GP practice replied and said that they were forwarding it to their clinical pharmacist for an opinion.
Two weeks passed, and I did not hear back from them. I emailed the practice again, but they told me they were still ‘waiting on his opinion.’
The rash got worse. In early August, I saw a private dermatologist in Hull. She gave me a GP request form. On the request form, the dermatologist asked my GP to prescribe me some Elocon cream for what she diagnosed as eczema. I emailed the practice the form, and that day they prescribed me the cream.
On August 12, 2024, the clinical pharmacist recorded the incident and the cream that he prescribed. However, he added a false statement claiming to have seen me. “Seen by clinical pharmacist” is what the record states. I haven’t spoken to him or met him. I have no idea who he is. He didn’t see me. It’s a false record.

A photo from medical records, which shows the false record of the pharmacist saying he “saw me”.
Retrospective Amendmendments
Incident 1

Incident 1: On December 8, 2023, I confided in a TEWV CMHT psychiatrist about a disturbing comment I had seen on my medical records in July 2022. My GP had entered, ‘Scan abnormal, to be expected, no further action,’ about an abnormal MRI neck scan that York Hospital detected in July 2022.
Two hours after I had seen the psychiatrist, the practice locked me out of my System One TPP online account. Three days later, when I got a new password, I saw the practice had amended the record. My GP surgery had added, “No review applicable,” to the record. They did not record who made the amendment, when they did so, or why.

A photo of the record that the practice retrospectively amended 18 months after they had recorded the incident.
They did this, in my opinion, to make up for the fact that they had neglected to investigate the abnormal scan eighteen months earlier.
Retrospective Amendements
Incident 2
Incident 2: I sought assistance for suicidal thoughts at York A&E on August 27, 2024. When the practice documented my visit to A&E, they left out important details. They entered, ‘Seen at accident and emergency, ongoing episode.’ However, they didn’t state anywhere on the record what that episode was or the reason that I went to A&E.

Medical records, which show the original entry did not state the reason I went to A&E. Suicidal feelings were omitted.
I blogged about it on my facial pain website: about the fact they had omitted critical information to downplay my mental health crisis. Three weeks after that, the practice went in and retrospectively added ‘suicidal feelings’ to the record. Since the date they added the “suicidal feelings” next to was August 27, you wouldn’t notice the amendment had been made if you looked at the record now.

Medical record, which shows how Ampleforth surgery added ‘suicidal thoughts’ weeks later, after I had blogged about this omission.
They didn’t document who did this, when they did it, or why.
Deleting and Re-entering Records

On 10th June 2024, I attended Scarborough Accident and Emergency Department for help with suicidal feelings. The secretary at the practice recorded this attendance twice. She entered, ‘Suicidal thoughts (ongoing episode), seen at Accident and Emergency (ongoing episode.)‘ The second record that she entered said, ‘Suicidal thoughts (ongoing episode,) mental health assessment (ongoing episode).’

Medical record, which shows how the practice recorded my visit to A&E on 10 June, 2024, with two entries.
I believe that she did this because she had seen that one of the leading GPs had deleted the record from one month previously on May 17th, 2024, so she was kindly protecting me from further deletions. Two weeks later, the leading GP went into my record and deleted one of those entries. They deleted the one which stated I had been to A&E.

The medical record shows how, two weeks later, a leading GP deleted one of those entries. There was just one left.
I wrote a post about this deletion on the My Facial Pain website, and two weeks later, the practice went into the record and re-entered the missing record. My GP practice did not record who did this, when and why.

The medical record shows how the practice re-entered the previously deleted entry. Here’s how the record now looks.
Omitting Critical Information

Incident 1: On 27th August 2024, I attended the Accident and Emergency department (A&E) at York Hospital for support with my suicidal feelings.
The practice omitted critical information in their recording of this incident. My GP practice noted the incident as “attended Accident and Emergency (ongoing episode).” But they didn’t explain what this ongoing episode was or why I went to A&E. Any future clinician who viewed my record would not have known that I went to A&E for help with suicidal feelings. This action, I believe, was to minimise my crisis.

Record showing how my GP practice omitted critical information about why I attended A&E.
Incident 2: On 7th February 2025, I tried to end my life. I was found unconscious on a golf course and taken to Cramlington Emergency Care Hospital, where I was admitted for 48 hours and where they administered IV NAC. “Glasgow coma state 13” was my conscious state.
Once more, the practice minimised the severity of my crisis by leaving out important details from the record. After I attempted suicide and Cramlington emergency care hospital admitted me for 48 hours for IV NAC, they wrote “seen at A&E” instead of “admitted”.

Medical record stating ‘seen’ at Accident and Emergency instead of ‘admitted.’

Disccharge summary from Northumbria NHS, showing that I was admitted and not ‘seen.’
I wasn’t “seen” at Accident and Emergency. I was admitted for 48 hours. The above discharge summary shows I was admitted on 7/2/25 and discharged on 9/2/25.
This record will lead future professionals to misjudge the seriousness of my attempt, as they will not see that I was admitted for emergency care.
Breaches of the Law

These breaches violate GMC guidance and the Data Protection Act 2018. They are not clerical errors—they are deliberate acts that obscure risk and undermine patient safety.
Good Medical Practice states that doctors ‘must’: 69) Make sure patient records are clear, accurate, contemporaneous (meaning recorded at the time of the incident), and legible. It states: 70) Patient records should include (f) decisions made, actions agreed and when/whether decisions should be reviewed and (g) who is creating the record and when. GMC guidance lastly states that doctors ‘must’ (71) keep records about patients in line with data protection laws.

GMC guidance: Good Medical Practice stating the principles of record keeping.
The practice’s actions have breached all of these principles. My GP practice has also violated data protection laws on the following articles:
- Accuracy Violation. UK GDPR Article 5 (1) (d) ‘Accuracy’ states that ‘personal data shall be accurate and, where necessary, kept up to date.’
- Transparency Violation. UK GDPR Article 5 (1) (a) Transparency states that ‘personal data shall be processed lawfully, fairly, and in a transparent manner.’
- Security Violation. UK GDPR Article 32, Security of Processing, states that ‘the controller shall implement appropriate technical and organisational measures to ensure a level of security appropriate to risk.’ If the practice have tampered with my records, they are not secure.
- Section 171 of the Data Protection Law 2018 makes it a criminal offence to alter, erase, or conceal personal data with the intent to prevent disclosure to the data subject or ICO.
Conclusion
Aside from the legal problems, Ampleforth Surgery’s actions have jeopardised my safety and overshadowed critical pathways for care and safeguarding. Concealing a patient’s suicide risk is extremely dangerous.
On a personal note, these experiences have been both devastating and terrifying. I’ve never felt fear like I have during these incidents. Every time I went into my record and saw that they had manipulated them again, I felt a level of threat that my mind and body had not previously experienced. I’ve also felt very alone about it because I have nowhere to turn for help.
A general practitioner is supposed to be a trustworthy advocate. However, Ampleforth Surgery has been a dangerous place from which I have had to stay away. This has shattered my trust in systems. Due to this practice’s ethical violations, I formally withdrew from their care on 2/9/25. I publicly announced my withdrawal from the practice and uploaded my withdrawal letter to X.

My letter of withdrawal from Ampleforth Surgery’s care, page 1.

My letter of withdrawal letter from Ampleforth Surgery’s care, page 2.
I have made it clear that I will not register with another GP until the ICO or another body has conducted a thorough audit trail of my records and corrected them to ensure that they are free of tampering and omissions.
Video 12: Advocacy Video Campaign
Photo Credits: Pixabay on Pexels. Open Clipart-Vectors, JS and Clker-Free-Vector Images on Pixabay.

2025-10-17 09:38
Northumbria NHS : A Critical Patient Safety Incident
Disclaimer: Northumbria NHS is not an attack on individual clinicians or institutions. This post exposes severe system neglect and patient safety violation. I am raising in the public interest to ensure that no one is left at risk in this way again. I am campaigning for urgent patient safety reform.
Trigger Warning: This blog post about Northumbria NHS heavily discusses suicide and mental health neglect, which some readers may find distressing. If you are struggling with your mental health and need support, there is a list of helplines at the bottom of this post. Please reach out for help if you are struggling. You are not alone.
In this blog post, I show a bottle of whisky that Northumbria NHS gave back to me after I survived a suicide attempt. The purpose of this is to expose severe systemic mental health neglect, not to promote self-harm.
Summary

Northumbria Specialist Emergency Care Hospital at Cramlington in Northumberland.
After surviving a fatal suicide attempt on February 7th, 2025, I experienced a critical and mind-shattering patient safety incident at Northumbria NHS that has left me profoundly shaken and vulnerable. This incident also raises serious questions about patient safety within mental health crisis care.
Context to Incident

On 7th February 2025, I attempted to take my life. This was the result of enduring twelve years of institutional harm and systemic neglect spanning across 19 NHS trusts, two local authorities, and a GP practice. The weight of it was too heavy to carry alone. So, I tried to commit suicide.
I sadly tried to end my life using a combination of Paracetamol, sleeping tablets and whisky. I passed out on a golf course in coastal Northumbria. As I understand it, two passers-by found me unconscious on a golf course and called an ambulance, which took me to Cramlington Emergency Care Hospital. I woke up in A&E twelve hours later. A nurse was yelling at me, saying that I was “lucky to be alive”. My conscious state is listed as “Glasgow Coma Scale 13” in my medical records.

The medical teams administered IV NAC for 48 hours. After 48 hours of treatment, the medical team confirmed that I had not incurred any damage to my organs and that I was ‘fit for discharge’.
Mental Health Assessment

Although I was physically fit for discharge, I was in a highly vulnerable mental state. I was still suicidal and confused and disorientated. The crisis team and psychiatric liaison team from Cumbria, Northumberland, Tyne and Wear NHS Trust (CNTW) assessed me. They concluded that I was still at risk and that they thought I required an inpatient hospital admission to a mental health unit.
CNTW informed me that TEWV (Tees, Esk and Wear Valleys Trust), my home mental health trust, was in the process of arranging an inpatient bed for me at Cross Lane Hospital.This is the audio from Nothumbria NHS, confirming an inpatient bed was being arranged by TEWV.
I didn’t believe this because the CMHT in Malton had discharged me in 2024, and they had refused a referral from the psychiatric liaison team five months later.
CNTW would not give me any concrete details about this admission. I repeatedly requested clarity from them about this bed, but they told me that TEWV would ‘call me later’. Northumbria NHS told me to make my own way back to Yorkshire. Neither CNTW or Northumbria NHS offered me any transport: ambulance or taxi to get back to Yorkshire. They gave me the discharge summary, which stated that TEWV was arranging an inpatient bed for me. They also made it clear to me that they had no further responsibility for my care.
However, there was no bed. TEWV told me later on the phone that they were not giving me any inpatient care, so Northumbria NHS misled me about that support.
Discharge summary from Northumbria NHS. It states that I still at risk and that TEWV were arranging an inpatient bed for me at my local hospital in Scarborough. This never happened.
Patient Safety Incident

When the ambulance brought me in to Cramlington Hospital, the ward took the bag from me with the remaining bottles of whisky and packets of paracetamol that I had used to try and end my life. As I was leaving the ward on Sunday, 9th February, the ward sister handed me back the carrier bag with a hospital sticker on it. In the bag were the two remaining bottles of whisky and the remaining packets of paracetamol that I had used to try and end my life two days earlier.
Northumbria NHS gave me back the whisky and the paracetamol that I had used to try and end my life: a fatal event that they had just spent 48 hours helping me to recover from.


I cannot communicate the shock I felt when I looked in that carrier bag. It was what their actions communicated. What Northumbria NHS was saying was, ‘Your safety and well-being are of no concern to us.’
Northumbria NHS offered me no transport and no local contacts. They offered me no directions and no concrete details of any follow-up care. And they handed me back the lethal substances that had led to me being found unconscious on a golf course and needing 48 hours of their emergency care. This incident was institutional abandonment and neglect at its most heinous.
This is what harm in healthcare looks like. This is what systemic abuse looks like.
Whitley Bay- The Spark

I found my way to a hotel in Whitley Bay, where I checked in for the night. Later that evening, I spoke to the crisis team at TEWV, who told me that there was “no inpatient bed”. Northumbria NHS “has got it wrong”, they said. This lie felt like a double betrayal. Either TEWV or Northumbria NHS had deceived me. I didn’t know which one. However, the fact remained that there was no inpatient admission for me, despite Northumbria telling me two hours earlier that there was.
They discharged me without any care and returned the lethal substances I had used to attempt to end my life. Is this what you call care? How could such critical errors and oversights go unchecked in an emergency care hospital?
February 9th, 2025, was the night that sparked the inspiration for my campaign. I couldn’t allow this level of abuse to happen to anyone else. And if I didn’t survive, I needed to create a paper trail documenting what had happened to me.

Mental Health Resources
If you are struggling and need help or support, please reach out to these organisations:
If you are in England:
Please call 999 if your need is urgent.
NHS 111 (option 2): Free 24/7 support available from trained mental health professionals.
Free phone Samaritans 116 123: Free 24/7 helpline for anyone in emotional distress. samaritans.org
Text SHOUT to 85258: Free, confidential 24/7 support via text with trained volunteers at giveusashout.org.
Mind – Call 0300 123 3393 or text 86463: Mental health information and support: mind.org.uk
Calm Zone (Campaign Against Living Miserably): 0808 585858: Open seven days a week from 5.00pm to 12.00 midnight.
National Suicide Prevention Helpline: 0800 587 0800
If you are in Scotland:
Breathing Space Helpline: 0800 83 85 87. Open Monday-Thursday 6.00pm-2.00am and weekends, Friday 6.00pm-Monday 6.00am
Scottish Association for Mental Health (SAMH): 0344 800 0550 or email info@samh.org. If you phone this number or email them, they will direct you to your local SAMH café where you can seek local peer support.
Photo Credits: Pixabay, Sam J Johnson and Shkraba Anthony on Pexels. Fawaz Buqammaz on Unsplash.

2025-10-17 09:17
TEWV: Betrayal and Broken Promises
Disclaimer: TEWV: Betrayal and Broken Promises is not a personal attack on individual clinicians or institutions. This post exposes serious mental health neglect in the public interest. I am campaigning for urgent mental health reform and improved crisis care so that no one else suffers what I have endured.
Trigger Warning: This blog post discusses suicide and mental health neglect that some readers may find distressing. If you are struggling and your need is urgent, please call 999. If you need support, please call NHS 111 (Option 2) or Samaritans free phone: 116 123.
In this post, I show a packet of Zopiclone. This is not intended to promote harm but intended to show systemic neglect – how a psychiatrist recommended the prescription of it long-term without offering or carrying out any review.
Summary
My previous post documented the immediate failings in the care provided by TEWV (Tees, Esk and Wear Valleys NHS Foundation Trust), leaving me with no support after surviving a suicide attempt in February 2025. This post documents serious systemic issues that I faced while I was under their care from March 2022 to March 2024.
Collusion

TEWV’s complicity in the harm that I have experienced across many NHS trusts has been a large part of their neglect, and it has what has made this narrative feel unsustainable. The additional pain that TEWV has inflicted on me is the way they have framed me as the problem.
On 8/12/2023, I confided in a CMHT psychiatrist about a disturbing comment on my medical records. My GP had written, ‘Scan abnormal, to be expected, no further action,’ about the abnormal MRI scan that York hospital detected in 2022.
Two hours after I saw the psychiatrist, Ampleforth surgery locked me out of my TPP online account. Upon regaining entry with a new password, the practice had added ‘no review applicable’ to the record. This timeline indicates that the psychiatrist phoned the GP and gave them the heads-up to alter the comment.

GP’s comment about the abnormal scan and underlined in red, is where the practice amended the record, after TEWV gave them the heads up to do so on 8/12/23.
In their discharge summary, TEWV wrote, ‘Felicia thinks NHS bodies are colluding with one another.’ I struggle to understand what the psychiatrist’s actions are if they aren’t collusion in covering up the situation and tampering with my records. But TEWV are framing me as the problem.

Discharge summary from TEWV, saying that I feel services are ‘colluding with each other.’
Denied Safeguarding
On March 6th, 2025, TEWV’s crisis team also told North Yorkshire County Council, (NYCC) to disregard a safeguarding request. The Care Quality Commission (CQC) asked NYCC to safeguard me from TEWV and my GP in February 2025, after my suicide attempt, which NYCC did close down. This constitutes institutional complicity.
The harm I have experienced is hard enough, but asking me to shoulder the responsibility for their complicity is too much to bear.
Reflection

This shocking timeline of events demonstrates collusion and a concerted effort to conceal clinical facts. It reveals that a TEWV psychiatrist was allegedly involved in prompting Ampleforth Surgery to immediately tamper with my medical records (specifically adding ‘no review applicable’) after discussing a key abnormality.
This action, alongside TEWV telling North Yorkshire County Council to deny me safeguarding and TEWV’s subsequent withdrawal of mental health support, illustrates the pattern of institutional complicity that has caused me sustained harm. This is a coordinated effort to frame the patient as the problem and shield institutional failure.
Cruel Behaviour

In August 2024, I presented at York A&E for help with my suicidal feelings. I saw a TEWV psychiatric liaison officer who assessed me at the emergency department. She referred me back to the CMHT for support. In November 2024, I saw a female psychiatrist at Princes Road Clinic, Malton, who in December 2024 told me that she was not going to provide any support or signpost me. The psychiatrist informed me that the referral was being closed.
That refusal of support was painful enough. But what was so unbearable was that she delivered this news to me wearing a smirk on her face. She was smirking as she told me that TEWV would not be offering me any further support. She seemed to be enjoying telling me this. It was sadistic and cruel.
Zopiclone

During that meeting in December 2024, I explained to the psychiatrist that I was having extreme difficulties sleeping. She made the decision to ask the GP to prescribe zopiclone, a sleeping pill, to me long-term. However, she didn’t see me again after this, so she recommended the prescription of Zopiclone without reviewing me.
Zopiclone is one of the medications that I used to try and end my life. This was reckless behaviour and showed no regard for my safety or wellbeing. And it was her doing all this while smirking that made her behaviour, in my mind, nothing short of inhumane.
Broken Promises

After surviving my suicide attempt in February 2025, TEWV gave me five outpatient appointments with their crisis team before they cut off all further support. One of those five appointments was with their team psychiatrist. I liked him. I found him to be warm, approachable and very human.
He listened, and he said to me, ‘Felicia, we need to come up with a plan. We need to sort your facial pain out,’ which told me that he understood that my physical pain was what had caused my suicidal crisis. This was the first time in twelve years that mental health services had acknowledged this.
The psychiatrist agreed to go through my medical notes and speak to the consultants at York Hospital to find out what was happening with my care and treatment. He promised to communicate with the medical consultants about how my facial pain affects my mental health.
I felt really hopeful. I thought that I may be turning a corner with this: that I finally had someone on my side.
Hiding Behind Bureaucracy

That didn’t happen. He didn’t do it. When I returned to see the psychiatrist, he said, ‘Sorry, it’s been difficult going through your notes.’ I interpreted this to mean, ‘There was too much to go through, so I didn’t bother.’ He told me that he had spoken with my GP and asked them to refer me to a new NHS trust to be reviewed instead.
His broken promises felt like a deep betrayal. By asking my GP to refer me back to the NHS trusts, he was sending me back to the dangerous merry-go-round that led to my suicidal crisis. His actions showed no regard for the cycle of harm I had endured, and it was a cowardly way of hiding behind bureaucracy.
The crisis team then cut off all further support. He left me with no plan or follow-up care after my attempt, and they told North Yorkshire County Council (NYCC) to close down the safeguarding concern that the Care Quality Commission (CQC) raised about me, which NYCC did do. They left me with no support when I was at my most vulnerable.
The merry-go-round

I will never, ever return to that merry-go-round. After my gaslighting experience at York Hospital and South Tees, I made it clear to my GP that I would not be attending any more medical appointments. I explained to them that I would not see anymore clinicians about my facial pain unless there was support or safeguarding in place to protect me from the institutional bullying. This is because of the excessive risk to my mental well-being.
Conclusion

The events that included a psychiatrist being complicit in the tampering of my records to conceal evidence, a second psychiatrist smirking at me while telling me that she is closing down a referral, prescribing zopiclone with no further review, a third psychiatrist promising to speak to medical consultants about my facial pain and then not doing so, and denying me care and safeguarding after surviving a suicide attempt amount to nothing short of mental health neglect.
This neglect is human rights abuse, and it goes wider than healthcare-related injustice. After surviving a suicide attempt, being refused protection or assistance goes beyond cruelty. Basic human rights include the right to access care during a crisis. TEWV’s denial of this care and treatment of me amounts to nothing less than institutional abandonment and human rights abuse.
The trust’s treatment of me has been cruel, degrading and inhumane.
Video 11: Advocacy Video Campaign
Photo Credits: Betzy Arosemena, Luis Alberto, Alexander Kriviskiy, and Majestic Lukas on unplash. Fotios Photos and Shkraba Anthony o
2025-10-17 08:47
TEWV: Silencing the Suicidal
Disclaimer: TEWV silencing the suicidal is not a personal attack on individual clinicians or institutions. This post exposes serious mental health neglect in the public interest. I am campaigning for urgent mental health reform so that no one else suffers what I have endured.
Trigger Warning: This blog post discusses suicide and mental health neglect that some readers may find distressing. If you are struggling and your need is urgent, please call 999. If you need support, please call NHS 111 (Option 2) or Samaritans free phone: 116 123.
Summary
TEWV (Tees, Esk and Wear Valleys NHS Trust) is my current mental health trust, under whom I have suffered prolonged harm and suffering. TEWV discharged me when I was a high suicide risk, and they have left me with no support following a suicide attempt that I survived in February 2025. This post documents the immediate failings with TEWV’s duty of care.
Context

I have been in a serious and sustained mental health crisis for six years. My mental health crisis is not an isolated incident or related to mental illness. My crisis is the result of both living with undiagnosed facial pain for this long and the institutional harm that I have suffered across so many NHS Trusts for 12 years. The magnitude and scale of the harm, and the absence of any appropriate support being in place have been too much to carry alone.
Discharged While I Was at Risk

In May 2024, the CMHT at Princes Clinic, Malton, discharged me. TEWV did this knowing that I was a high suicide risk. They also discharged me without doing any new assessment, and they gave me no warning that they were withdrawing their support. The CMHT did not discuss it with me first. They just wrote to me to tell me they had discharged me from their care.
TEWV knew, following repeated discussions that I had had with one of their mental health nurses, that I was suffering with chronic suicidal ideation. They therefore discharged me unsafely when I was at risk.
Denied A&E Support

On 10th June, 2024, I attended Scarborough A&E for help with my suicidal feelings. I saw a psychiatric liaison officer from TEWV. He told me that I could return to A&E for mental health support again. I told him that I felt actively suicidal, but he said, ‘You cannot come back. This service is for emergencies only.’ I’m not sure what being actively suicidal is if it’s not an emergency.
He then told me to self-refer back to the CMHT and to North Yorkshire County Council, whom he knew had both closed my file and discharged me. The TEWV officer said this, knowing full well that a patient cannot self-refer to either of those services. They require a professional referral, so this guidance was misleading and dishonest.
This rejection was a kick I had not experienced before. TEWV blacklisted me from going to A&E at Scarborough hospital for mental health support.
Refused Internal Referral

In August 2024, I attended York Hospital A&E for help with suicidal feelings. I saw a female psychiatric liaison officer from TEWV. She was a pleasant lady. She did an assessment, and she told me that she was re-referring me back to the CMHT in Malton for support.
The CMHT at Princes Road clinic assessed me in November 2024, but in December 2024, they told me that they were not providing me with any support, nor signposting me anywhere for help. They gave me no reason why they were denying me any mental health support.
It was self-defeating that TEWV refused a referral from one of their internal psychiatric liaison officers. TEWV boycotted an internal referral, which highlights how nonsensical their bureaucratic processes are. That’s secondary to how negligent they are to deny a patient mental health support after an A&E officer has urgently referred them back to the CMHT for support.
Abandoned After My Suicide Attempt

On 7 February, 2025, I tried to end my life. After years of institutional harm from numerous NHS trusts, I had been hovering in a state of suicidal ideation. However, it was the conglomeration of TEWV’s, North Yorkshire County Council and Ampleforth Surgery’s neglect that pushed me to try to commit suicide.
I couldn’t hold the heaviness of TEWV withdrawing their support, North Yorkshire County Council withdrawing my social care support and my repeated discoveries that Ampleforth surgery was falsifying my medical records. It was too much.
The shock and the trauma were too much to hold. I had nowhere to turn for help with it. I felt desperately alone and frightened, and I wanted to go.
Misled about an Inpatient Bed

I took a large overdose out in the open in coastal Northumbria. As I understand it, some people found me unconscious on a golf course, and I woke up twelve hours later in A&E at Cramlington Emergency Care Hospital. After they administered IV NAC for 48 hours, CNTW assessed me. They said that I was still at risk and that I needed an inpatient admission. They confirmed that TEWV were arranging an inpatient bed for me at Cross Lane Hospital. The audio clip below records this conversation I had with the CNTW crisis team in Northumbria.
The discharge summary from Northumbria NHS also states that a bed was being arranged for me.
Discharge summary from Northumbria NHS, stating that I was still at risk and that TEWV were arranging a bed for me on an inpatient ward.
On 9th February, after Northumbria NHS discharged me, TEWV told me on the phone that there ‘was no bed’. There was no inpatient admission. They misled me. The crisis team at TEWV gave me five outpatient appointments at Cross Lane Hospital and then cut off all further support.
On 6th March, 2025, the crisis team at TEWV also told North Yorkshire County (NYCC) to close down the safeguarding concern that the Care Quality Commission, (CQC) raised on my behalf. This did lead to NYCC closing down the concern and taking no action. As a result of TEWV’s action, I was left with no safeguarding when I was deeply vulnerable and at risk.
It has been nine months since I survived my suicide attempt, and TEWV has left me with no support and ensured that I have been denied any safeguarding by NYCC. It is inhumane and cruel.
Conclusion

I can’t put words to how it feels to have had no mental health support for this long. And to have been denied safeguarding. I wish Northumbria NHS had left me unconscious because I’ve woken up to more abuse from TEWV than I went to sleep with. Things are worse than they were before I tried to go.
Being denied mental health support after surviving a suicide attempt is like being thirsty and not being able to get a drink of water. It gets harder as the days pass. The thirst deepens. That thirst translates into a numbness I have never experienced before. I cannot feel who I am anymore.
It’s also horrific knowing I cannot even go to A&E at Scarborough for support. I can’t go anywhere for help. I’m trapped. If I go an A&E department for help in another location, they will likely liaise with TEWV, who will control and manipulate the narrative.
I think the lasting memory of TEWV is what one of their crisis team nurses said to me at one of my five outpatient appointments in February.
She asked if I had any further plans to end my life. I told her I did. I told her what they were. She said, ‘You want to keep your cards close to your chest, because if you tell us your plans, I’ll have to write it in your notes, and we’ll scupper your chances. Keep things quiet and you’ll succeed.’
I’m really not joking.
It’s incomprehensible.
The silencing of the suicidal.
Video 10: Advocacy Video Campaign
Photo Credits: Ron Lach and Alex Green on Pexels. Hasan Almasial, Andreea Popp and Mehrpouya on Unsplash. Copyright Free Pictures on Pixabay.

2025-10-12 06:53
Manchester Royal Infirmary: Deliberate Inaction
Disclaimer: This post about the Manchester Royal Infirmary is not an attack on individual clinicians or institutions. It is exposing a pattern of systemic neglect and institutional harm that I have suffered. I am campaigning for systemic reform and an end to systemic neglect.
Summary

The Manchester Royal Infirmary, like many other NHS trusts, failed to help me when they could have. Like all the other trusts, I saw three relevant departments: ophthalmology, oral maxillofacial surgery and ENT.
However, in spite of being one of the best hospitals in the country for head and neck services, they deflected responsibility back to Guy’s Hospital and the North Manchester General and did nothing. The Manchester Royal Infirmary was the hospital of neutrality and deliberate inaction. Here’s what happened:
Ophthalmology

The surgeon who performed my superficial parotidectomy asked my GP to refer me to ophthalmology regarding my ongoing periocular pain. I was also suffering from post-parotidectomy facial nerve palsy at the time and was unable to close my left eye.
In 2019, I consulted a highly regarded ocular plastic surgeon at the Manchester Royal Infirmary. I was really hopeful that she might help me because of her extensive experience and her reputation.
However, this oculoplastic surgeon saw me once and discharged me. She did no investigations: scans or blood tests regarding my periocular pain. She did diagnose my left astigmatism which was due to failed eye closure. However, regarding my longstanding eye pain, she deflected responsibility to the oral maxillofacial surgery department and included North Manchester General in the internal referral.
The Legacy from Leeds

It was palpable from the first and only meeting that she wanted to get rid of the case. She noted from the medical records that I had previously consulted a highly regarded professor at St Thomas’ Hospital regarding my ptosis, a matter she seemed reluctant to discuss.
She was also aware that the UK’s leading oculoplastic surgeon at Leeds Teaching Hospitals had dismissed me in 2014. As I state in both my video and blog post, that incident at Leeds Teaching Hospital accounts for why future ophthalmologists dismiss me so quickly. That professor set the precedent for the narrative of medical neglect that has played out, particularly with ophthalmology. The Manchester Royal Infirmary was a classic example of this.
I was disappointed. I liked her. She was a pleasant individual, and I genuinely believed that she had the potential to assist me. It was another lost opportunity.
Oral and Maxillofacial Surgery

I saw two oral and maxillofacial surgeons in a joint consultation at the Manchester Royal Infirmary. Again, they were both very experienced head and neck surgeons who had the potential to assist me with the ongoing pain in my remaining parotid gland. Either of them had the experience necessary to remove the rest of my gland.
The issue of my post-parotidectomy paralysis was less prominent. Thanks to the input of a physiotherapist at The Lindens Clinic in Timperley, my facial function was slowly returning.
Deflection of Responsibility

However, regarding my ongoing facial pain, their response was devastating. They spent two hours aggressively quizzing me about my symptoms. I felt intimidated and disbelieved about my facial pain. They offered me no treatment solutions or were willing to do any investigations. Firstly, they recommended that I return to the Salivary Gland Unit at Guy’s Hospital, which they said should perform a new sialogram and compare it to the one they did in 2017.

Letter from an oral maxillofacial surgery surgeon at MRI deflecting responsibility for my care back to Guy’s Hospital.
The oral maxillofacial team at the Manchester Royal Infirmary also referred me back to the North Manchester General, to the infectious diseases department. They requested that the team at North Manchester General conduct further diagnostic testing on my parotid tissue, which they had stored in their fridge. They asked them to test my tissue for rare infectious diseases like Bartonella and stated that I needed to remain under this team for my care.

Clinic letter from the oral maxillofacial team at MRI deflecting responsibility for my care and referring me to infectious diseases at North Manchester General Hospital.
However, the infectious diseases team at the NMG refused to do those tests on my tissue and discharged me after one appointment. Both hospitals left me with no care or treatment options.
Head and Neck Services, ENT

It was the head and neck team at Chorley Hospital (Lancashire Teaching Hospitals) that referred me to the head and neck team at the Manchester Royal Infirmary. Among the many NHS trusts that saw me once and subsequently referred me onwards was Lancashire Teaching Hospitals.
Once more, the head and neck surgeon I saw at the Manchester Royal Infirmary in late 2019 was a very skilled medical professional who had more than he needed to assist me.
Things got off to a strange start. While I was waiting for the surgeon to collect me, the nurse passed me. I was sitting in the corridor outside his consulting room, and she dropped my notes by accident.
My notes landed face up, and I saw a green medico-legal form that the Manchester Royal Infirmary had filled in. This is a form that medical teams fill out to defend themselves against a medical negligence claim. I had not seen a solicitor about any claim. I became aware that this trust was already on the defensive when I saw that medico-legal form. I felt cautious as I entered the consultation. The surgeon did not know I had seen this, but I had. And I couldn’t unsee it.
Botulinum Toxin Injections

The surgeon did have a glint of compassion in his eye, but I could also sense the guilt in his demeanour. He was aware that both his colleagues and the system had failed me.
The consultant gave me a token gesture instead. He didn’t do any investigations, but he offered me botulinum toxin injections for my facial pain. Botulinum toxin is used in the treatment of many facial pain disorders by producing temporary skeletal muscle relaxation. In pain management, botulinum toxin has an analgesic effect by reducing muscle hyperactivity. I have refused Botox injections for clear reasons.
My Reasons For Refusal

I have no diagnosis. Therefore, we do not know what we are treating. Botox is a dangerous chemical that can have serious side effects. I do not, therefore, want a clinician injecting chemicals into my face when we do not know what the cause of my pain is.
If you walk into a doctor’s surgery with a rash on your hand and the doctor says, ‘I don’t know what it is, but we’ll try lavender oil.’ The oil has the potential to help, but it also has the potential to exacerbate the rash. This is because the doctor is suggesting lavender oil for a rash that hasn’t been identified or diagnosed.
There is a high chance that Botox injections could make my condition worse. If infection is the cause of my pain, then there is a high probability that Botox would worsen my symptoms.
The rheumatologist who I saw in 2015 tried oral prednisolone, which is a steroid. Oral prednisolone made my symptoms far worse, so I do not want to take this risk. I am not being an ‘obstructive’ or ‘difficult’ patient. I have refused Botox injections because I do not want to accept chemical injections when we do not know what the injections are treating.
Conclusion

The Manchester Royal Infirmary did nothing. It was deliberate inaction. They chose, like many others, deflection and neutrality. As I mentioned in my post about York Hospital, I think that the MRI took no action, because to diagnose and intervene would have meant getting their hands dirty in a messy case.
It would have meant acknowledging the harm and neglect not just within their trust but across the entire network of NHS trusts, so they chose neutrality and left me in pain. It was easier.
My story is a political one. It’s not about me. It’s not about my pain, my suffering, or a human being asking for urgent help. It’s about politics – policy crossfire – about large institutions protecting reputations, shielding failures, and refusing to act because action would expose the scale of neglect.
Manchester Royal Infirmary didn’t fail to help. They chose not to help because helping would have meant shining a light on the system itself: a system that puts self-protectionism and silence before patient care and patient safety.

Photo Credits: Drew Beamer and Olga Guryanova on Unsplash. Tima Miroshnichenko, Isa QuePereira, Thirdman and Pixabay on Pexels.

2025-10-12 06:29
York Hospital: Ignored Abnormalities and Deflection
Disclaimer: This post about York Hospital is not an attack on individual clinicians or institutions. I am disclosing serious systemic neglect that I have expereinced in the public interest as part of my campaign to push for patient safety reform.
Summary

York Hospital is the last hospital I attended. I was a patient there from 2022 to 2023. York Hospital identified clear abnormalities regarding my facial pain condition via MRI scanning, but they took no action. They disregarded the clinical findings and neglected to provide me with an explanation. Furthermore, they shifted the responsibility to South Tees, who also failed to take any action.
As a way of not having to deal with the findings, a clinician at York Hospital gaslighted me in a way I have never experienced before. This experience has made it impossible for me to attend any further medical appointments since. This is what happened:
Ear, Nose and Throat

I saw an ENT consultant in June 2022. Like all of his preceding colleagues, he promised to help me. He consented to perform an MRI and a CT scan, intending to compare them with the scans conducted by NHS Lothian. The consultant committed to investigating the root cause of my facial pain. He stated in his clinic letter that he was determined to ‘get to the bottom of this.’ I felt hopeful and optimistic.

Clinic letter 1 from the ENT consultant at York Hospital.
Deflection of Responsibility
I had an MRI neck scan and a CT neck scan in July 2022. Two weeks after I had the scans, this ENT consultant wrote to me to tell me that they had found an abnormality in my retromolar area and buccal fat pad region. I felt helpless and devastated when I read his letter. He told me that he had sent the case up to South Tees instead of dealing with it internally.

Clinic letter 2 from the ENT consultant confirming they found an abnormality.

Clinic letter 3 from the ENT Consultant, deflecting case up to South Tees.
The ENT consultant said that oral maxillofacial surgery needed to deal with the abnormality, not ENT, and because oral maxillofacial surgery at York Hospital had rejected my GP’s referral in 2022, he had transferred the case up to the max fax team in Middlesbrough.
He met his match with the consultant at James Cook Hospital, who sent the case back to him. South Tees told York Hospital that they found the abnormality, so the ‘ball was in their court’. The two hospitals sent my case back and forth for months but neither of these hospitals took responsibility for the problem. I felt like a tennis ball that had been batted off pitch.
My Head Pain

What was so difficult about this situation was that my left-sided head pain was worsening. It feels, and it still feels, like someone is screwing a corkscrew into the top of my head. My ear pain was also becoming more acute with this feeling of fullness in my left ear that I have. I asked the ENT consultant about my head pain. He said he thought it was an enlarged temporal bone causing the pain. The consultant said he would investigate it, but he didn’t. He discharged me from his care and gave me no answers or treatment options for the pain.
Ophthalmology

My experience with the ophthalmology clinic at York Hospital was equally as dismal. They too ignored clinical findings and declined to help me. I had been to the ophthalmology clinic at York Hospital about my periocular pain in 2014. This was after the ophthalmologist at Leeds Teaching Hospital kicked me off the ward and stopped my medication. The ophthalmology department at York Hospital also dismissed me back in 2014.
I attended ophthalmology at York Hospital in 2022 and I asked the ophthalmologist about the radiology images from the MRI scan that ENT did. I asked him about my small left eye and the swelling that I could see at the left side of my head. Additionally, I asked him if my pain and the visible swelling could be temporal arteritis. He said it wasn’t. He told me that what I was seeing was ‘just the angle of the scan’. Really?

MRI neck scan, 2022, York Hospital. Small, less bright left eye.




“Treatment Nil.”
Then he really upset me. When I asked him to explain what the cause of my periorbital pain was. He said, ‘The issue is with the tissue.’ His comment exposed that he knew that my medical problem is a soft tissue problem, but he did nothing about it. “Treatment nil,” he wrote in his clinic letter.

Clinic letter from ophthalmology acknowledging abnormal radiology findings, but stating ‘treatment nil.’
He did acknowledge that the abnormality that ENT had found on the MRI scan needed following up. He wrote to oral maxillofacial surgery and asked them to see me. But his defensiveness and unwillingness to address my periorbital pain were, I think, an act of protection. He knew I saw his colleague back in 2014, and he did not want to acknowledge that I had a medical issue with my left eye because to do so would have exposed his colleague’s medical negligence.
Oral Maxillofacial Surgery

What took place with oral maxillofacial surgery at York Hospital was utterly horrific. The trauma I experienced with this department has prohibited me from being able to attend any further medical appointments for my facial pain.
In 2022, the oral and maxillofacial surgery department rejected my general practitioner’s referral, stating that the case was “too complex.” But after ophthalmology referred me once more, they agreed to see me. In February 2023, I had an appointment with an oral maxillofacial surgeon at York Hospital.
I asked him to explain what this abnormality was that they found, but he refused to give me an explanation. He moved on from the question and gave me no answers.

Radiology report, showing abnormality in buccal fat pad and pterygoid muscle region. Still unexplained.
A Patient Safety Incident
I then showed him some of the radiology images from that MRI scan. I told him that where the white is, is where I have the pain. He gaslighted me and tried to make out I was seeing things. ‘It’s just a coincidence that you’re seeing that. You’re choosing to see it,’ he said.



Photoshopping My Images
I then showed him one of the radiology images where there is white all around my left eye and down to my jaw. I told him that the associated pain I experience is located here. He told me that the image was simply the “angle of the scan” and was therefore “inaccurate.”
After this, the situation became sinister. He displayed this picture on his computer and applied photoshopping to make all of the white show up on my right side. ‘Look, Felicia,’ he said. ’I can make it come up on the other side.’ It was like sitting next to the magician, Paul Daniels.

The radiology image that surgeon photoshopped in front of me.
I lastly showed him some of the CT radiology images from NHS Lothian. I asked him to explain the visible asymmetry in my face, to which he replied, ‘The quality of your I-pad is shit.’ It was difficult to believe what I was hearing. You just don’t expect this kind of conduct from clinicians. Even the nurse looked shocked.

CT neck radiology image from NHS Lothian that I asked this surgeon to explain.
The following is what made this type of gaslighting so horrible: gaslighting is bad at any time. It’s awful when medical professionals minimise a patient’s symptoms and claim they’re all in your head. But when they have clinical evidence in front of them that there is something wrong and continue to tell you that you are imagining it and manipulate that data, it’s profoundly sinister.
Why Did They Do It?

I’ve said on this blog and in my social media video campaign that my story is a dirty institutional cover-up that involves two local authorities, 19 NHS trusts, and a general practitioner’s office.
If York Hospital had acted on the abnormality that they found in 2022, it would have exposed, in their view, failings at previous trusts. The hospitals that would have been most sorely implicated are Leeds Teaching Hospital, Guy’s and St Thomas’, The North Manchester General, The Manchester Royal Infirmary, Charing Cross Hospital, NHS Fife and NHS Lothian. It was easier, therefore, to gaslight me and deflect responsibility. That’s why I think they did it.
Impact on Me

I was in a seriously bad way after this consultation with profound trauma. I suffered extreme insomnia for months, and I was woken up in the middle of the night with flashbacks of that consultation. Following this gaslighting incident, I decided that I was not going to attend any more medical appointments because the risk to my mental health was way too severe. I cancelled all follow-ups with York Hospital and have not seen any clinicians about my facial pain since this incident.
Questions For York Hospital

My campaign video below asks York Hospital many questions about my condition and about the associated radiology images. The most important question is what was the abnormality that they found on the MRI scan. The other questions I ask York Hospital are:
a) whether my soft tissue is now completely calcified and whether my pterygoid muscle is now damaged on the left side. The radiology report states the abnormality has extended there and something doesn’t look right in these images.




b) what is the swelling and pain next to my left eye if it isn’t temporal arteritis?


c) whether the visible enlargement above my left frontal lobe is indicative of neuroinflammation.




d) I also ask questions about the visible white patches on my left lung and whether these could be an associated infection.


In spite of asking York Hospital these questions on X, (formerely Twitter) they have not replied to my questions.
Conclusion

What took place at York Hospital – the gaslighting, the deflection and the delays – was appalling. When you know a patient is in this much pain and has been suffering for this long, then you should act on any abnormal findings immediately. They chose not to. This has caused me immense suffering and is a miscarriage of justice. It also violates many of the principles set out in Good Medical Practice, particularly those concerning doctors’ obligation to answer questions honestly and provide patients with the information they want and need in a way they can understand.
My experience at York Hospital was a serious patient safety incident that raises questions about the urgent necessity to make patient safety a reality in hospitals. It is currently merely a politically correct slogan that politicians use when it is convenient. However, my experience at York shows that the reality for many patients is a long way away from the patient being safe and cared for. Ignoring an abnormal scan is not patient safety. It is patient danger.
My pain is being prolonged, and diagnostic clarity is being delayed. Accurate diagnosis is a critical component in patient safety.
I strongly feel that York Hospital’s behaviour and actions are complicit in and colluding with a long-running cover-up that has lasted for twelve years. They took no action. They ignored the abnormal clinical findings because to name it-to diagnose and intervene would have meant acknowledging the harm not just within their walls, but across the entire network of NHS trusts. So they chose neutrality and deflection.
But neutrality in the face of harm is not care. It’s complicity. I would never be able to walk through the doors of York Hospital again after this experience. Never.
Video 9: Advocacy Video Campaign
Photo Credits: Ksenia Chernaya, Karolina Grabowska and RDNE Project on Pexels. Click-free-vector-images on Pixabay. Buddha Elemental, Ira Pavlyakovich and Hermes Rivera on Unsplash.

2025-10-12 06:09
South Tees: My Gaslighting Nightmare
Disclaimer: Gaslighting at South Tees is not an attack on individual clinicians or institutions. This post documents serious systemic failings and institutional harm. It is in the public interest; I am drawing attention to this neglect as part of my campaign to push for systemic change so that no one has to experience what I have.
Summary

Gaslighting at South Tees was horrific and terrifying. I experienced medical gaslighting at James Cook Hospital by two powerful male clinicians, consecutively.
Both gaslighting instances left me questioning my judgement and my sanity. They left me in a state of acute distress and delayed me getting treatment for my facial pain condition. Additionally, they participated in the cycle of cover-ups, responsibility deflection, and institutional bullying that I have become entangled in for twelve years. This is what took place at South Tees:
Oral Maxillofacial Surgery

I saw an oral maxillofacial surgeon at James Cook Hospital, South Tees, in 2022. I took the radiology images from NHS Lothian with me to my appointment. As I mentioned in the previous post, I was unable to get answers to my questions regarding these scans because the ENT surgeon at NHS Lothian declined to provide me with a follow-up consultation. I still had questions about the visible asymmetry in my face.
He was shifty and defensive from the off. He didn’t like the case—I could tell—and I found his manner threatening from the minute I walked into the consultation room. I felt I was in the presence of an army officer, not a doctor. Even the accompanying nurse in the room looked frightened.
I showed the surgeon the CT radiology images on my iPad from NHS Lothian. I asked him if he would explain the visible asymmetry and the dense areas of white on the left side of my face, as I have been wondering if these are areas of calcified tissue. Below are some of my radiology images that I showed him.




The exchange that then took place was frightening. He told me that the asymmetry that I was seeing in the images was because ‘my face was lopsided in the scanner.’
Firstly, my face was in a cage during these scans. It was not lopsided. Secondly, these scans were done in 2022, two years previously, in Edinburgh. This surgeon is based in Middlesbrough, and he did not see me go into the scanner. So how could he know if my face was lopsided?
The Joker

My gaslighting nightmare at South Tees was diabolical. The clinician’s attempt to pull the wool over my eyes made him seem like a joker. I remember him as a joker because of that. A sinister clown. It is well known to all patients and healthcare providers that a radiologist will not allow a patient to enter a scanning machine unless they are positioned in the centre.

This consultant insulted me and questioned my intelligence. He gaslighted me and attempted to silence me because he didn’t want to deal with my medical issue. He then rudely told me to “live with the pain” and “stop shopping around”. This abuse is more than just gaslighting. It’s institutional bullying. “Shopping around” is not what I’ve been doing. I’ve been showing up at a lot of new clinics because NHS trusts keep closing my file.
Broken Promises

The surgeon told me that he would “get to the bottom of my problem”. In his clinic letter to my GP, he stated that he would “leave no stone unturned in finding a diagnosis”. He promised to look into my persistent head pain by performing an MRI of my brain and parotid gland. However, two weeks after seeing the surgeon, he wrote to me telling me that he had cancelled the scans and discharged me.
This incident hurt. He raised my hopes about someone who was willing to help, and then, like the others, he smashed those hopes. This surgeon left me with no alternative care or means of treatment when I was in pain.

A letter from the surgeon promising to ‘leave no stone unturned in finding a diagnosis’. He did not ‘turn over any stones’. He discharged me 2 weeks later.
Infectious Diseases

My experience with the infectious diseases consultant at James Cook Hospital, South Tees, was even worse. I saw him a few months later. I asked him to explain why these antibiotics that I have been taking for twelve years subdue my symptoms when I am on them, but when I come off them, my pain returns.
In his dismissive reply, he claimed that the antibiotics were a “placebo effect”. The placebo effect is when a patient’s physical or mental health improves after receiving a “fake” treatment, such as a sugar pill, simply because they believe it will work and expect to feel better. He was basically saying to me that my mind or brain is convincing my body that this fake treatment is the real thing.
This interaction was deeply insulting. Firstly, it was insulting to the doctors who have been prescribing these antibiotics, as it questions their judgement. It was also insulting to me. I am not imagining the therapeutic effects of these tablets. They are the only medication that quells my pain, and to reduce my reality to an imaginary effect was deeply offensive and degrading.
No Investigations

This consultant’s arrogance was vile. He made this grossly insulting comment, but he didn’t do any blood tests or investigations of his own. He also failed to take into account the blood test findings over the years. Numerous blood tests have revealed elevated MCHC, WBC, RBC, haemoglobin count, and neutrophils. These are significant clinical findings that require explanation because they suggest that my illness is infectious.
Below is a selection of blood tests that different hospitals did at different times over the years. They all exhibit the same elevated WBC, MCHC, and neutrophil markers.






He did not, however, take note of all those discoveries. This rendered his remark regarding the antibiotics being a “placebo effect” irresponsible and contemptuous.
Good Medical Practice

This kind of gaslighting that I experienced at South Tees violates many principles set out in Good Medical Practice. The General Medical Council (GMC) sets out key principles in its guidance, which asks doctors to:
– Make the care of patients their first concern.
– Respect every patient’s dignity and treat them as an individual.
– Listen to patients and work in partnership with them, supporting them to make informed decisions about their care.
– Act with honesty and integrity, and be open if things go wrong.
– Protect and promote the health of patients and the public.
– Never unfairly discriminate against patients or colleagues.
– Never abuse patients’ trust in you or the public’s trust in your profession.[i]

Sections 23 and 28 from Good Medical Practice.

The Doctor-Patient Relationship

Gaslighting of this nature undermines these principles, and it defies the principles of what a doctor-patient relationship is. The Doctor-Patient Relationship Toolkit, which is published by the British Medical Association, provides ethical standards that clinicians are supposed to uphold when relating to and with their patients.
Healthcare professionals are among the most trusted and respected groups in society. The onus is principally on the healthcare professional to make contact with patients work well.
The BMA
The toolkit’s key principles are:
- Doctors must make the care of patients their first concern.
- Good communication requires openness, honesty and an ability to listen.
- Good patient care is person-centred and takes into account the patient as a whole person.[ii]
Conclusion

The gaslighting that I experienced at South Tees does not in any way comply with the above principles set out by the GMC or the BMA. It’s an antidote to the fundamental principles of what doctoring is. Their behaviour contradicts the principles of kindness, care and respect. In the medical field, gaslighting has become commonplace. It is accepted as OK. But it is not OK. It is not what healthcare is about.
It’s time that gaslighting is properly challenged. Clinicians need to be guided to act with far greater grace and compassion, and they need to be made aware of the risks of their actions. My gaslighting experiences at South Tees were deeply traumatic. They have had a long-lasting impact on me, particularly in relation to becoming hypervigilant. I now go into medical appointments, expecting clinicians to gaslight me.

Gaslighting in healthcare is dangerous, especially when a powerful male clinician does it to a vulnerable woman. I felt silenced. I felt frightened, and I felt unable to challenge both clinicians. Gaslighting is an insidious form of abuse. It can leave a patient in a high-anxiety state, suffering with both confusion and insecurity.
Most critically, gaslighting prolongs the patient’s suffering by delaying diagnostic outcomes and delaying the delivery of urgent medical treatment.
Medical gaslighting can represent a significant risk to patient safety, contributing to diagnostic errors and disparities in care. It undermines patient safety and trust, and hospitalists have a unique opportunity to lead in reforming this aspect of care.
The Hospitalist.
Footnotes
[i] The BMA: Ethics Toolkit: The Doctor-Patient Relationship, February 2025. https://www.bma.org.uk/
[ii] The BMA: Ethics Toolkit: The Doctor-Patient Relationship, February 2025
Video 8: Advocacy Video Campaign
Photo Credits: Sven Ciupha, Sohail Nawaz, Akram Huseyn, Chuttersnap, the National Cancer Institute and the National Institute of Allergies and Infectious Diseases on Unsplash. Yankrukov and Alexander Krivitskiy on Pexels.

2025-10-01 01:08
NHS Lothian: My Story of Dehumanising Treatment
Disclaimer: This post about NHS Lothian is not an attack on individual clinicians. It is raising awareness about the dangers of systemic discrimination and delayed care in the public interest so that no one else endures what I have survived.
Summary

NHS Lothian was, by far, the worst experience I have had of an NHS trust. I have been deeply impacted by the harsh and dehumanising treatment I received while I was a patient at NHS Lothian.
A surgeon at NHS Lothian stonewalled and silenced me. I faced outrageous prejudice and discrimination, and I experienced a lack of duty of candour in response to my complaint. This is what happened at NHS Lothian:
The odds were not in my favour

The ENT department at NHS Fife referred me to head and neck services at NHS Lothian about my left facial pain. They had found an enlarged masseter muscle on my left side. The odds were stacked up against me before I even arrived at NHS Lothian. The referring surgeon at NHS Fife sent the new surgeon at Lothian the discriminatory letter that a psychiatrist in Fife had written about me. I knew I was heading for trouble. I could feel it in my bones.
It’s important to say that at this time my left ear pain was acute. I was in agony with a feeling of fullness in that ear. I also developed a banging sound in that ear, pulsatile tinnitus, which was like sound attacks in my head.
Stonewalled & Silenced

I saw the surgeon at NHS Lothian in July 2020. He planned to perform some scans to look at my parotid gland. The surgeon told me that he would see me again after the scans to find ‘a way forward’. I asked him if he would refer me to ophthalmology about my periocular pain and infectious diseases. He said he would do both.
One week after I saw the consultant, I had an MRI scan of the brain, an MRI of the neck, a CT scan of the neck and a bone scan. I never heard from him again. The surgeon ignored me for 18 weeks. It was horrific and so painful. I wrote to him three times. I requested a follow-up consultation from him; however, he did not respond.
He did refer me to NHS Fife pain management, but they refused to see me. He also referred me to the infectious diseases team, who discharged me after two appointments despite finding abnormality in two blood tests. Being ignored by this surgeon for eighteen weeks was so painful, and it was made worse by the fact that I was living with worsening ear pain.
Obscene Discrimination

The ENT surgeon, who I saw, wrote an inappropriate and discriminatory comment about me on a radiology request form. On the request form for a CT scan, which he sent to the radiology team, the surgeon wrote, ‘Be careful with this one. The patient has significant psychiatric problems.’
The dehumanising way that NHS Lothian treated me was fundamentally rooted in this comment.

This is the radiology request form, on which the surgeon at NHS Lothian wrote the discriminatory comment about me.
I was absolutely horrified and appalled when I saw this comment. Firstly, this man had met me once. He didn’t know me, and secondly, whatever his judgements were about me, they had no place to be written on a radiology form that was to investigate pathology in my parotid gland, where pathology had previously been found both at Guy’s Hospital and North Manchester General Hospital.
The surgeon’s discriminatory comment is also a breach of the Equality Act 2010, which protects certain groups from discrimination.
No Duty of Candour

The biggest punch from NHS Lothian came in their response to my complaint. I complained to them that the surgeon had promised to see me again to find a way forward but that he refused to give me a follow-up consultation. I complained that he had left me with worsening ear pain and no resolution for eighteen weeks.
After a long delay, they replied by telling me they were closing my file. NHS Lothian told me to go to NHS Fife pain management to deal with my pain. They gave me this instruction knowing that NHS pain management had refused to see me. It was their surgeon who had referred me to NHS Fife pain management. He had received their refusal letter, so he knew.

This is the response from NHS Lothian to my complaint about the surgeon not giving me a follow-up consultation and telling me to go to Fife Pain Management.

This is the letter from NHS Fife Pain Management to the surgeon at NHS Lothian telling him that they had refused to see me. They had received this six weeks before responding to my complaint.
I was left with no options for care or future steps after this trust led me down a dead end. It was just devastating. I was stuck in a corner with no way to get help, helpless.

Professional Duty of Candour

Their response to my complaint was a breach of the Professional Duty of Candour, published by the General Medical Council and the Nursing and Midwifery Council.
The Professional Duty of Candour states that:
- Every health and care professional must be open and honest with patients and people in their care when something that goes wrong with their treatment or care causes, or has the potential to cause, harm or distress.
This means that health and care professionals must:
- tell the person (or, where appropriate, their advocate, carer or family) when something has gone wrong
- apologise to the person (or, where appropriate, their advocate, carer or family)
- offer an appropriate remedy or support to put matters right (if possible)
- Explain fully to the person (or, where appropriate, their advocate, carer or family) the short- and long-term effects of what has happened.[i]
NHS Lothian did not do any of the above. Critically, they did not offer any support or explain why the surgeon refused to offer me a follow-up consultation, which is a basic tenet when delivering care to a patient. It is unreasonable to refuse to see a patient again, especially when the patient has written to you three times with questions about their condition.
The surgeon’s refusal to answer my questions was also a breach of Good Medical Practice, which states that doctors must:
- 23. (a) Answer questions honestly.
- 28. Give patients information they need and want in a way they can understand. [ii]
He did neither.
My Request to NHS Lothian

I am making a request to NHS Lothian to remove the discriminatory comment from the radiology request form. I am requesting this because the comment has no place there, and it is breeding systemic bias against me. That comment is now on my radiology records. If a new NHS trust requests those scans from NHS Lothian, they will see the surgeon’s comment, and it will cause them to view me negatively.
I am also asking NHS Lothian to answer my questions about the scans that they did. I did not get any answers to my questions because of the surgeon’s refusal to give me a follow-up consultation.
My questions are:
What is the visible asymmetry in my face?


What are the large areas of intense white around my cheekbone? Is it calcified tissue?

Has my nasalis tissue and muscle now started to wear away?


Is my orbital and cheekbone now damaged, as it looks different on the left side?


Conclusion

My experiences at NHS Lothian were not only dehumanising. They were damning. They involved denial of care for no reason, discrimination, silencing and a violation of guidelines about candour. Their conduct left me feeling alone and with nowhere to turn.
Delays in care, outright discrimination, and a lack of accountability pose significant risks. They force a patient to live with undiagnosed pain for longer than is necessary, which deepens both physical and mental suffering. This conduct is cruel, and it is not what healthcare is about. Healthcare is about curing people of illness and disease, and their ruthless treatment of me serves as a critical warning for them to re-evaluate how they treat patients.
FootNotes
[i] The General Medical Council and The Nursing and Midwifery Council, (joint guidance): Openness and Honesty when Things go Wrong; The Professional Duty of Candour, June, 2015
[ii] The General Medical Council: Good Medical Practice, January, 2024.
Video 7: Advocacy Video Campaign
Photo Credits: Thirdman and Mart Production on Pexels. Alexis Fauvat, Andreia Cunha and Milos Tomsevic on Unsplash.

2025-09-28 07:13
Dangerous Discrimination at NHS Fife
Disclaimer: This post about my experiences at NHS Fife is not a personal attack on clinicians or institutions. It raises the serious issue of systemic mental health discrimination in healthcare in the public interest. This post is calling for the end to stigmatisation in healthcare and equal access for all to healthcare services.
Summary

In 2020, I experienced an incident of dangerous discrimination at NHS Fife that not only shattered my trust in the system but which has profoundly affected me and my outlook on the world and people.
What happened was a devastating violation of my integrity at NHS Fife. A psychiatrist—who had never met or spoken to me—accessed my records and wrote a letter claiming I have factitious disorder, stating my facial pain is “made up to feed the need to have a sick role”.
Context

In 2019, I fell into a mental health crisis. My crisis was caused by living with unrelenting facial pain for years. The incessant obstacles with NHS trusts who refused to see me about my facial pain condition also prompted my crisis. On top of my pain was the frustration regarding clinicians finding abnormal pathology but refusing to act on those findings. The combination of all three factors pushed me into a crisis state that I had never experienced before.
In 2020, I made a naive and foolish decision. I moved up to Fife, thinking that I may get a better shot of receiving medical treatment from surgeons up in Scotland. I arrived in Fife in crisis and accepted a two-week respite admission into Whyteman’s Brae Hospital from the mental health team.
Upon returning to the community, I received support from a community psychiatric nurse (CPN), who visited me on a weekly basis. This support was instrumental in helping me cope with the distress I was experiencing due to my untreated facial pain. I did not have a psychiatrist.
A Cruel Twist of Fate

My GP referred me to head and neck services at NHS Fife for my facial pain. I saw an ENT consultant in November 2020 at The Victoria Hospital in Kirkcaldy. He agreed to do some scans and refer me to tertiary head and neck services in Lothian. After I had the MRI scan in November 2020, I returned to see him in January 2021.
I could never, in a million years, have seen this stab in the back coming. This consultant told me that he had a letter from my psychiatrist. I had no psychiatrist.
He received a letter claiming that my facial pain was purely “fictionalised”. I asked the ENT consultant who this psychiatrist was, and I had never heard of the person. It transpires that a psychiatrist in Fife who had never met me or spoken to me accessed my records and wrote and published a letter that said that I am making up my facial pain ‘to feed the need to have a sick role’.
He sent this letter to multiple agencies in Fife.
Denial of Care
As a result of this letter, both NHS Fife and NHS Lothian denied me access to care for my facial pain. NHS Fife Pain Management refused to see me. They rejected a referral from Head and Neck Services at NHS Lothian. And an infectious diseases consultant also discharged me and took no action regarding two blood tests which both showed raised infection markers.

Letter from NHS Fife Pain Management stating that they refused to see me following a referral from NHS Lothian.

A blood test done by infectious diseases at NHS Fife in November 2021, which showed raised infection markers. No action taken.

A blood test done by infectious diseases in November 2021 at NHS Fife, which showed raised infection markers. No action taken.
This denial of care from NHS Fife left me to live not only with unresolved physical pain, but it also left me lost in a cloud of fear, confusion and victimisation that is difficult to put into words.
My Medical Records

Thankfully, this psychiatrist’s discriminatory diagnosis has not been entered onto my record summary in England or Scotland. However, having that discriminatory letter on my records whilst I was living in Scotland was terrifying.
In Scotland, their system of digital record keeping is called Sci-Gateway, and it is different from System One in England. Sci Gateway allows any medical consultant in secondary care to have instant access to all of your records and correspondences. This ability to see a patient’s full records is more challenging for secondary clinicians to do in England. This means that when I went to Accident and Emergency, called 111, or attended any outpatient appointments in Scotland in secondary care, clinicians could easily see that letter.
This reality made living in Scotland terrifying. Whenever I attended any medical appointments, the stigmatisation and discrimination were a given. As soon as the second lockdown lifted, I left and moved back to England.
Personal Impact

This incident was a violation of my integrity and a deep betrayal. It took courage to leave a home of 16 years in England and move up to Fife in search of medical help. This letter scuppered my chances of receiving that medical help. The medical profession viewed me as a fruitcake after he published that letter. The publication of the letter resulted in systemic discrimination and stigmatisation, which is a very frightening form of bullying and exclusion to experience. I felt trapped and alone, like I had nowhere to turn.
Legislation Against Discrimination

The Equality Act 2010 is in place to shield protected characteristics from direct and indirect discrimination. My experience of being denied medical treatment for a physical condition due to discrimination was a breach of this legislation.
The Equality and Human Rights Commission also confirmed that this letter is potentially a breach of two of my human rights. They confirmed that it was potentially a breach of Article 8: The Right to Privacy (which includes protection of one’s personal and psychological integrity) and Article 14: The Right to Protection from Discrimination.
The General Medical Council

General Medical Council in central London. They regulate and discipline the country’s doctors.
I raised a complaint about the psychiatrist’s actions with the GMC. My complaint was simple: the psychiatrist wrote a damaging and discriminatory letter without ever meeting or speaking to me. His letter had led to NHS trusts denying me treatment for my facial pain.
The GMC opened a provisional enquiry into my complaint. This is an initial investigation.
They found that the psychiatrist who wrote this letter had gone through my notes. He had noticed that when I had been in Whyteman’s Brae for the two-week respite break, the duty psychiatrist, whom I saw twice, had written in my notes that he thought I was making up my facial pain. That is where I got the information from.
The GMC did not find the psychiatrist unfit to practise. That wasn’t an issue for me.
Lack of Transparency
My issue was that the GMC was not fully transparent with me. I complained to the GMC that the psychiatrist wrote this discriminatory letter without ever meeting me or speaking to me.

My complaint to the GMC about the psychiatrist Fife, stating he wrote a letter about me without having met me or spoken to me.
They found that he had taken his information from my notes. In their final report, the GMC stated in their summary that I had complained that the psychiatrist wrote this letter without evaluating my clinical records.

The final report from the GMC demonstrates how they reworded my complaint to state that I said he “wrote a letter without adequate assessment of records.” This is not what I said.
This was not what I said. I said that the psychiatrist wrote this discriminatory letter without ever meeting me or speaking to me.
The GMC’s conclusion that the psychiatrist had based his information on an earlier record did not bother me. It was their lack of transparency regarding the details of my complaint that concerned and upset me. They changed my wording.
The GMC’s alteration of the wording in my complaint—specifically, their assertion that I had complained about the psychiatrist ‘not looking in my records’—was inaccurate and appeared to manipulate my complaint to align with their narrative. I found this alteration to be disheartening and dishonest.
Duty of Candour
The General Medical Council are the publishers of The Professional Duty of Candour. The GMC set the standards for doctors behaving honestly. They are not setting an example if they are not completely open and honest with the public. If the GMC asks medical professionals to respond to complaints with candour, then it is critical that they act openly and honestly with the public. I would hesitate to approach them again now.
Conclusion

Discrimination and misdiagnosis in healthcare are dangerous. They lead, as in my case, to denial of healthcare for physical conditions that need intervention and treatment.
The Department of Health must tackle stigmatisation in healthcare. It’s not enough for Good Medical Practice to say that doctors must not ‘discriminate against patients’.
Integrating stigma awareness training in hospitals and GP practices is an essential pathway to tackling discrimination. It will ensure that everybody within the protected groups of the Equality Act has equal access to healthcare.
The elimination of stigmatisation and discrimination will also ensure that we have a fully inclusive healthcare system that does not marginalise patients based on bias and prejudice.
It’s time for change.
Video 6: Advocacy Video Campaign
Photo Credits: John, Elliot FZ, Alexas Fotos, Ekaterina Bolovtsova and Pavel Danilyuk on Pexels. Irwan on Unsplash.

2025-09-18 01:48
Charing Cross Hospital: My Missing MRI Images
Disclaimer: This post about Charing Cross Hospital is published in the public interest. My campaign is not a personal attack on individuals or institutions but an effort to expose serious patient safety failures and systemic neglect. I am asking for this discrepancy to be formally investigated.
Summary

The Charing Cross Hospital is one of the medical centres where I suspect clinical evidence may have been concealed as part of an institutional cover-up. It’s at this hospital where there are unanswered questions about my missing MRI images. Here is what happened:
The Scans

My then GP referred me to a head and neck surgeon in the ENT department at Charing Cross Hospital about my left-sided facial and ear pain. I saw the surgeon on May 23rd, 2019. This was one year after my superficial parotidectomy at The North Manchester General.
This surgeon did four scans. He conducted an MRI scan of my neck, an MRI of my brain, a CT scan of my neck, and an ultrasound of my neck.
After I had had the four scans, I was sitting with the surgeon in his consultation room. He was looking at my radiology images on three large screens. He enlarged an image, and I could see huge white globules on the left side of my face where I have pain.
I asked the surgeon if the globules were calcifications because the histology report one year before had shown calcified tissue in my parotid gland. He said “no”, and he turned off his computer. I asked him to turn back his computer three times. He refused. The surgeon proceeded to tell me that the previous surgeon had removed most of my parotid gland.
He became decidedly aggressive, and he told me that my pain was ‘psychological’. I walked out.
Los Angeles

I flew over to Los Angeles shortly after to see a head and neck surgeon who confirmed there is still 70% of my left parotid gland remaining. He confirmed there is still some of the superficial lobe and the deep lobe, and there is some accessory parotid tissue over the masseter muscle. He also confirmed there are still calcifications in my gland.
The Disc

After I got back from Los Angeles, I requested the disc with my four scans on from Imperial College NHS Trust. But when I got the disc, I noticed that three of the scans—the CT neck, the MRI brain, and the neck ultrasound—had file icons next to them, but the MRI neck scan had no icon next to it.

Image showing missing MRI neck scan file
An orange message that read “error decoding image” appeared when I clicked on the MRI neck.

This is the sign that came up when I clicked on the MRI neck scan.
Something wasn’t quite right.
I telephoned Imperial College NHS Trust. I enquired as to why there were no MRI neck scans on the disc, and they told me they had “merged the MRI brain and MRI neck scans”.
However, after carefully reviewing the radiology images on the disc, I cannot find the images that I saw on the surgeon’s screen on May 23rd, 2019. I cannot see the MRI images of the big white globules on the left side of my face. I cannot see the images in question anywhere on the disc.
What I Think has Happened

I am not making any accusations. Although I cannot be certain, I think that the trust has possibly concealed some critical information. I think that Charing Cross Hospital did merge the two scans. However, I think that when they merged the two scans, they possibly deleted some of the radiology images that I saw as part of an institutional cover-up.
Why would they do this? If they found an abnormality on the MRI neck scan, they may not want to expose the failings at the North Manchester hospital, which should have removed the entire gland and performed further diagnostic testing. Additionally, new abnormal findings could expose the possible lack of transparency that I suspect took place at Guy’s Salivary Gland Unit in January 2017.
Information Commissioner’s Office

This incident is about truth, transparency, and the right to a correct diagnosis.
This missing data is not a minor administrative issue—it may contain vital diagnostic information that could help me reach an accurate diagnosis for a complex and ongoing health condition.
I am asking that the Information Commissioner’s Office (ICO) investigate this issue. If Charing Cross Hospital has deliberately concealed clinical evidence, then I would like it revealed. The clinical information will assist me in getting a diagnosis and the correct treatment.
I did publicly request that the Information Commissioner’s Office (ICO) investigate this. I asked them on X (formerly Twitter), but they responded with deflective stonewalling. They told me to contact PALS at Imperial College NHS Trust. Their action of deflecting responsibility to PALS was dishonest. PALS do not have the power to uncover the potential deletion of some of my radiology files.
The Integrity of Our Healthcare System.

This incident is bigger than just one case—this is about the integrity of our healthcare system.
This isn’t just a case of poor care — it raises serious concerns about the integrity of medical records and the transparency patients are entitled to under the UK Data Protection laws. When there is vital clinical evidence missing or potentially concealed, the consequences go far beyond one patient. It undermines the entire system.
Conclusion

Radiology data transparency is a cornerstone of patient safety and diagnostic integrity. If a hospital withholds, alters or deletes imaging records, it undermines clinical decision-making and exposes patients to misdiagnosis, delayed treatment and avoidable harm. Transparent access to radiology findings ensures continuity of care, enables second opinions, and protects patients from institutional gaslighting. Therefore, an investigation into my missing MRI images at Charing Cross Hospital is essential.
Video 5: Advocacy Video Campaign
Photo Credits: Ivan Samkov and Mart Production on Pexels. National Cancer Institute, Towfiqu Barbkuiya, Kreative Kwame Venti Views on Unsplash.

2025-09-17 11:39
North Manchester General Hospital: An Uncompromising Position
Disclaimer: This post about The North Manchester General Hospital is not a personal attack on individuals or institutions. I am exposing a serious and systemic pattern of neglect in the public interest. I am campaigning for systemic and patient safety reform so that no one endures what I have survived.
Summary

My story at the North Manchester General Hospital was another missed opportunity to get a diagnosis and treatment for my condition. It was also the hospital that left me in an uncompromising position.
An oral maxillofacial surgeon performed a superficial parotidectomy in 2018, but he didn’t do a scan beforehand. He went in blind. He removed some of the gland, but there is still 70% remaining. The histology showed parenchymal damage and sialolithiasis. Because I came through surgery with severe facial nerve palsy, I cannot find a surgeon to remove the rest of my diseased gland. This means I am living with excruciating pain on a daily basis.
Oral and maxillofacial surgery

I saw an oral maxillofacial surgeon in 2018. The surgeon agreed to remove the superficial lobe of my parotid gland, but he did not do a scan first. He operated blind. He relied on the clinical findings from Guy’s Hospital, which had found glandular malfunction. I woke up from surgery with severe facial nerve paralysis, which recovered in four months.


The histology showed dense secretions in the ducts, calcified tissue, and reactive lymph nodes. The parenchyma was sialolithiasis.

The histology report from my parotid gland surgery at The North Manchester General Hospital in 2018.
I benefited from the section he did remove with a reduction in my pain levels. But unfortunately, I still have 70% of my damaged gland remaining. I saw a head and neck surgeon in Los Angeles one year later who confirmed via CT scanning that there is still some of the superficial lobe and the deep lobe, and there is some accessory tissue over my masseter muscle. The duct is also still connected to the gland. The surgeon did not cut the duct and tie it up.

Report from Los Angeles showing the areas of my parotid gland that still remain following surgery at the North Manchester General in 2018.
Uncompromising Position

However, I cannot find a surgeon who will remove the rest of my gland. I have seen nine different surgeons in the UK. They have all said they will not remove the rest of my gland. Their decision is because of the risk of further facial paralysis, which they say could be permanent if they perform a revision parotidectomy.
The North Manchester General Hospital has left me in an uncompromising position. If the surgeon had done a scan before performing surgery, he would have seen the pathology, and he could have referred me to a surgeon who was more confident to remove the entire gland.
No Tissue Culture

The other missed opportunity was the refusal by both the surgeon and Infectious Diseases to culture my parotid tissue. They did do a standard pathology report, but six months after my surgery the Oral Maxillofacial department at the Manchester Royal Infirmary wrote to the Infectious Diseases team at the North Manchester General. They asked them to culture my tissue and do further tests to look for rare infectious diseases like Bartonella infection. But they refused. I saw an infectious diseases consultant at the NMG once and also asked him to do these tests, but he said no.

The letter the Manchester Royal Infirmary wrote to The North Manchester General asking them to test my parotid tissue for rare infectious diseases like Bartonella.
A Missed Opportunity

This was a major missed opportunity to detect what bacteria is potentially causing this infection. The North Manchester General Hospital had my parotid tissue in one of their medical-grade freezers. They could have easily done further tests on my tissue, but they didn’t.
Their refusal to culture my tissue is particularly frustrating in light of the fact that the surgeon who performed my surgery knew that infection was the cause of my pain. He wrote in his discharge summary under diagnosis: repeated infections in the left parotid gland. Therefore, his and his colleagues’ refusal to culture my parotid gland tissue felt reckless and unyielding. Why did the surgeon decline to perform additional tissue testing to identify the bacteria causing the infection if he was aware that it was an infection?

A diagnosis from the North Manchester General Hospital stated in the discharge summary: repeated infections in the parotid gland.
Request for Reconsideration

A patient with a diseased parotid salivary gland. Vector illustration of sialolithiasis.
This post serves as an urgent call-out to the head and neck surgical world to reconsider your decision to perform a revision parotidectomy. I fully understand the risks involved in repeat surgery, but I cannot live with this pain any more. I have also explained in the footage below that if you were to perform surgery, I would sign a disclaimer to accept responsibility for any risks of either temporary or permanent facial nerve palsy.
Conclusion

Life scientist researching in a laboratory. A scientist examines biopsy samples.
When rare infections go undiagnosed for years, every missed opportunity is significant. The failure of North Manchester General to culture my parotid gland tissue represents more than mere clinical oversight. It was a denial of diagnostic clarity. In cases like mine, where symptoms persist and standard tests fall short, advanced diagnostic techniques like metagenomic sequencing can be life-altering.
The longer rare pathogens remain unidentified, the greater the risk of misdiagnosis and irreversible harm. This review on rare infectious disease diagnostics outlines why timely, precise testing is essential.
Video 4: Advocacy Video Campaign
Photo Credits: Artem Beliaikin, National Cancer Institute, Maria Kovalets and Manuel Bonadeo on Unsplash.

2025-09-15 10:16
Guy’s and St Thomas’: Discharged Too Soon.
Disclaimer: This post about Guy’s and St Thomas’ is not a personal attack on individual clinicians or institutions. I am exposing a serious and systemic pattern of neglect in the public interest. I am campaigning for systemic reform so that no one endures what I have survived.
Summary

My experience at Guy’s and St Thomas’ NHS Foundation Trust was a missed opportunity to receive an accurate diagnosis and appropriate medical treatment for my condition. In 2016, three departments—Ophthalmology, Oral Maxillofacial Surgery, and Infectious Diseases—all identified abnormalities related to my facial pain.
However, they all disregarded the clinical findings and took no action. They all discharged me prematurely, leaving me in pain and providing me with no answers, care, or treatment options. This is what happened:
Ophthalmology

I saw a professor of ophthalmology in 2015 at St Thomas’ Hospital. He diagnosed my left ptosis. He told me that my left levitator had collapsed, but he took no action to look at what had caused this collapse to happen.

My left ptosis was diagnosed at St Thomas’ in 2015.
The professor also told me that my periocular pain is a problem with the soft tissue. His comment indicated that he knew that I have an infection or inflammatory problem around my left eye, but he did not do anything to help me. Despite this knowledge, he did nothing.
The professor discharged me after three appointments, advising me to ask my GP to refer me again for corrective ptosis surgery once my symptoms had subsided. However, my symptoms have yet to improve.

A clinic letter from ophthalmology in 2015 at St Thomas’ stating they were discharging me. He discharged me too soon.
Infectious Diseases

I saw an infectious diseases consultant in October 2016 at St Thomas’ Hospital. He was rude and aggressive with me; I remember that. I also remember having severe pain, a stiff neck, and chills at the time. He did two blood tests; both showed high infection markers, notably, raised neutrophils.
However, he disregarded the clinical findings. The consultant gave me no answers or treatment options. He ignored the findings and belittled my symptoms. He also had the evidence on file that ophthalmology had diagnosed my left ptosis. However, he made no enquiries about this abnormal finding or the links between those findings and his blood tests.
Instead, the consultant made a futile suggestion that I see a chronic fatigue specialist, which had no relation to the clinical findings or to my symptoms. I wasn’t suffering with fatigue. I was in pain. It is my belief that the consultant knew that this was a complicated soft tissue infection (SSTI.)
Oral Maxillofacial Surgery

The biggest issue occurred at the Salivary Gland Unit at Guy’s Hospital, where I was a patient from January 2015 to February 2017. I saw an oral maxillofacial surgeon in January 2015 who found glandular malfunction in my left parotid gland. He found an obstruction in my gland and duct via sialography. They washed the obstruction away, which gave me four days of relief, but my symptoms returned shortly after that.
He also did a blood test which showed raised infection markers, notably with my neutrophils, and an MRI scan which detected enlargement of my left parotid gland.

Blood test from Guy’s Hospital, showing abnormal infection markers.
In July 2015, an ultrasound showed mucous plugging in my gland, which is a thickening of saliva and a form of obstruction. A registrar then performed a sialendoscopy in December 2016, which showed a heavy thickening of saliva and obstruction. The registrar washed out my gland and put me forward for ongoing washouts every six weeks.
A Strange Turn of Events

There was then a strange unfolding of events that has left me with unresolved questions.
One month after I had seen the registrar, the lead dental radiologist at the Salivary Gland Unit carried out a second sialendoscopy in January 2017. The radiologist reported that “everything was normal.” The Salivary Gland Unit then discharged me from the clinic, having promised me regular washouts only one month previously.
Lack of Transparency

I am not making any accusations. However, I think that it is a possibility that the lead dental radiologist wasn’t transparent about the clinical findings from that sialendoscopy in January 2017. Here’s why I think that: The salivary gland unit found obstruction and mucous plugging in my parotid gland in 2015. The clinic letter from the Salivary Gland Unit in 2015 states this. The registrar then found further obstruction in 2016.

Clinic letter from The Salivary Gland Unit at Guy’s Hospital in 2016, stating they had found an obstruction in my left parotid gland.
The histology report from my superficial parotidectomy at The North Manchester General Hospital in 2018, one year after Guy’s Hospital discharged me, showed abnormality in my parotid gland tissue. One of the anomalous findings was the presence of dense secretions in the ducts. The abnormality discovered by the salivary gland unit at Guy’s in 2015 and 2016 is exactly the same as this clinical finding. It’s therefore odd that the investigation that the dental radiologist conducted in 2017 was deemed “normal”.

A clinic letter from the Salivary Gland Unit in 2017 stating that everything was ‘normal’ and that no further treatment was required.

A histology report from 2018 at The North Manchester General showing dense secretions in the ducts.
I also think that it’s possible that if the radiologist has been telling the oral and maxillofacial surgeons I have been seeing that “everything was normal”, that could be the reason they discharged me after just one visit. This potential lack of transparency has possibly created a form of collusion around the ‘there is nothing wrong’ narrative.
A Missed Opportunity

My experience at Guy’s and St Thomas’ NHS Foundation Trust was heartbreaking. They missed an opportunity to diagnose and treat my condition. The trust could have diagnosed and resolved my condition back in 2016. Three departments had clinical information at their disposal that showed there was something clinically wrong. However, instead of communicating across departments and acting, they discharged me and left me in pain.
Accountability

I am seeking answers and accountability from Guy’s and St Thomas’ about why all three departments discharged me from their care when they found abnormal clinical findings. It is important for me to know why they did not do more to help me. I am also asking the Salivary Gland Unit for their transparency about those clinical findings from January 2017.
Being honest about clinical findings isn’t just a matter of professionalism – it’s a cornerstone of patient safety. When clinicians withhold or distort diagnostic information, it delays treatment, deepens suffering, and erodes trust in the entire healthcare system. This isn’t about an administrative error – it’s about integrity, accountability, and the right of every patient to receive timely, accurate care. As this article from Patient Safety Learning explains, diagnostic delays are often rooted in poor communication and cognitive bias, and the consequences can be life-altering
Video 3: Advocacy Video Campaign.
Photo Credits: Claudio Shwartz and Chad Stembridge on Unsplash. Markus Winkler and Fotios Photos on Pexels.

2025-09-15 10:28
Leeds Teaching Hospitals: The Ground Zero of My Medical Journey
Disclaimer: This post is not a personal attack on individuals or institutions. I am exposing a serious and systemic pattern of neglect in the public interest. My campaign is for systemic reform so that no one endures what I have survived.
Summary
My medical story begins at the Leeds Teaching Hospitals. It was also the beginning of the legacy of medical neglect and the beginning of my medical journey. In 2014, a professor of ophthalmology found and diagnosed an infection. He admitted me for 48 hours of IV antibiotics, but he then discharged me without doing a blood test first to see if the infection had improved.
He also ordered my GP to stop my antibiotics. Because of his carelessness, doctors have denied for years that my illness is due to an infection. Also, his actions have had a knock-on effect on the way future ophthalmologists have viewed me. Numerous ophthalmologists around the UK have dismissed me. This one decision that the professor made has set off a cycle of years of neglect.
This is what happened at Leeds Teaching Hospitals:
Ophthalmology

My facial pain condition began in 2013. It was triggered by a flea bite to my left eyelid. Orbital cellulitis was the initial diagnosis, and severe orbital pain was my main issue. I saw a professor of ophthalmology, an oculoplastic surgeon at Leeds Teaching Hospital, in January 2014. He detected and diagnosed me with an infection via two blood tests. Both showed raised infection markers. His clinic letter to my GP clearly states that infection is the cause of my pain.

A clinic letter from 2014, written by a professor of ophthalmology, stating that infection is the cause of my condition.

One of the 2014 blood tests that revealed infection was performed by the ophthalmology professor.
The professor of ophthalmology admitted me for 48 hours of IV ciprofloxacin and oral linezolid. At the end of those 48 hours, he discharged me, and he provided me with no follow-up care. He didn’t do a repeat blood test to see if the infection had improved before he discharged me. The surgeon also wrote to my GP at the time and told them to prescribe no more antibiotics. After he discharged me, my condition severely worsened. I got very sick, and my pain worsened.
I was also forced to seek help privately, and this care cost me £18000 of borrowed money, which bought me antibiotics and blood tests under the care of a private rheumatologist in London for two years. After receiving treatment at a private hospital, my condition stabilised.
Domino Effect

Since this incident in 2014, I have seen over five ophthalmologists about my periocular pain. I have seen them at different clinics at various NHS Trusts, but they have all discharged me after one appointment with no treatment or answers even when they have identified and detected abnormal clinical findings.
Oral Maxillofacial Surgery

In 2022, my GP referred me to oral maxillofacial surgery at Leeds Teaching Hospitals for my left-sided facial pain in the remaining left parotid gland. My GP sent the referral to a named clinician at the oral maxillofacial department. It was York Hospital who instructed him to refer me there.
Leeds Teaching Hospitals refused the referral and did not give me a reason why they would not see me. Oral maxillofacial surgery discharged me without even seeing me.
Accountability

This is how one poor decision can lead to a systemic failure of care. These decisions that Leeds Teaching Hospital made have had a critical impact on how my medical journey has unfolded. If they had made different decisions back in 2014, I am convinced that I would not have faced this 12-year diagnostic delay.
I would like answers and accountability from Leeds Teaching Hospital about why they made these poor decisions. Accountability and openness are crucial to a patient’s healing after they have been harmed by the healthcare system.
In order to guarantee safe healthcare and patient safety, accountability and transparency are also essential. I am therefore asking Leeds Teaching Hospital to be accountable for their actions and decisions.
Video 2: Advocacy Video Campaign
Photo Credits: Tom Wilson on Unsplash. Fernando Capetillo and Brett Jordan on Pexels

2025-08-06 08:10
An Update From Felicia
TW: This post discusses suicide, which some readers may find distressing. If you are in the UK and need support, please contact 111, option 2, or the Samaritans freephone on 116 123.
An Update From Felicia

An update from Felicia: It’s been 5 months since I last wrote a blog post. I’ve missed posting on here. During this time, I’ve been reflecting on various topics and gathering ideas that I’m eager to share. I hope to reconnect with my readers and explore new themes that resonate with us all.
My silence wasn’t because I’ve had nothing to say. I survived a fatal suicide attempt in February 2025, and I have been dealing with the haunting aftermath of being left with no support by Tees, Esk and Wear Valleys Trust, North Yorkshire County Council and my GP. I’ve faced a wall of silence from them all. I’m not at this stage going to divulge into the details of my suicide attempt. However, the triggers to my attempt to end my life were living with undiagnosed facial pain for 12 years coupled with the cruelty and abject neglect that I have faced from so many NHS bodies. It has been, and continues to be, too much to carry alone. The universal abandonment and blacklisting from the NHS has left me with nowhere to turn.
This experience has compelled me to advocate for better mental health support and to raise awareness about the importance of accessibility and compassion in our healthcare systems. It is essential that those who are struggling feel heard and supported, rather than abandoned in their darkest moments.
A Wall of Silence

The services who were meant to care have given me no help since surviving my suicide attempt. No outreach. No support. Nothing: just stone-cold neglect. It’s been a reckoning. And it’s hurt and continues to hurt. It’s been a daily challenge trying to piece myself together amidst the isolation. So, that’s the reason for my absence on here. I’ve been trying to stay alive, which hasn’t been easy.

This neglect not only exacerbates existing issues, but it also deters others from seeking help, fearing a similar fate. It is crucial that we unite our voices to demand change, ensuring that mental health services are not just available but also responsive and empathetic to the needs of the community.
Video Advocacy Campaign

Over the last four months, I’ve been working on an advocacy video campaign to further my cause. Unfortunately, a small WordPress website like this just hasn’t been getting me enough reach, so I’ve decided to try a new medium – video. I’ve filmed and produced 16 videos which document the failings that I have experienced across various NHS trusts in the UK regarding their denial of care for my facial pain and for my mental health crisis.
I am hoping that these videos will help me to get the diagnosis and intervention that I need for my facial pain and accountability for what has happened to me. Most importantly, I hope to promote change. The inspiration behind my campaign is to push for safer healthcare and much greater patient safety in hospitals across the UK. I want to see a healthcare system where transparency and accountability are at the forefront of our system. That’s what I want to see.
I am posting these videos daily on TikTok and X (formerly Twitter). In one month, I will have an archive presentation of them on YouTube and Vimeo. I will also be posting them on here. Over the next month, I will now be writing shorter blog posts about the failings I have experienced across the NHS with my videos. I will then, hopefully, return to writing blog posts about the wider issues that I enjoy writing about, such as patient safety in healthcare and an update on my campaign and journey forward with my facial pain.
Thank you for your support and patience.

Video 1: Advocacy Campaign
Photo Credits: Timeklife, Shamble Studios and Bernard Hermant on Unsplash.

2025-02-06 03:47
The NHS Trusts Involved In My Case
Disclaimer: The Public Interest Disclosures Act 1998 ‘protects workers from detrimental treatment or victimisation from their employer if, in the public interest, they blow the whistle on wrongdoing.’[1] Whilst I am not an NHS worker, I am naming the NHS Trusts that have been involved in my case because I believe that this story is of public interest. My story has involved 19 NHS trusts in the UK, who have failed to diagnose and treat my condition over a 12-year period.
The total number of trusts includes 16 NHS trusts regarding my facial pain and 3 mental health trusts. This has been a miscarriage of justice. I do not want this to happen to anyone else. I am naming the NHS bodies with the intention not to slander or be defamatory but because I want to promote better care for others and because I want to see a move towards real patient safety.

The NHS Trusts
MY NHS Number; 439 021 8999
Complaint; Undiagnosed acute left-sided facial, periocular, ear and head pain.
Calderdale and Huddersfield NHS Foundation Trust
The Calderdale Royal Hospital
July, 2013; Ophthalmology
Initial Diagnosis of my condition was Orbital Cellulitis. It was triggered by a flea bite to lower left eyelid. I had raised WBC, neutrophils and I quickly developed connected pain and swelling around my left eye and cheek.
Bradford Teaching Hospitals NHS Trust
Bradford Royal Infirmary
August, 2013; Accident & Emergency; Ophthalmology
I saw an ophthalmologist re my acute orbital pain, who thought it was blepharitis. She prescribed me Maxitrol Steroid eyedrops, which treat eyeball inflammation. I had a severe reaction to these eye drops. My condition significantly worsened after using them. The pain and swelling around my cheek and eye began to involve the left side of my head.
Leeds Teaching Hospitals NHS Trust
Aerial photo showing the St James’s University Hospital known as Jimmy’s.
St James’s University Hospital
2nd December 2013 – 28th January, 2014; Ophthalmology
I saw an ocular plastic surgeon, who I consulted with twice in January 2014. He did a Lyme disease test, which was negative, and an MRI scan of my orbits, which he said was normal.
The ophthalmologist did two blood tests that showed raised infection markers, neutrophils, and ESR. He said that clinical ‘evidence points to an infection as the likely cause, likely Staphylococcus aureus.’ He tried oral doxycycline, which didn’t work. The ocular plastic surgeon then admitted me for 48 hours of intravenous antibiotics on 24th January discharged me on 28th January, 2014.
During the time that I was on the infection control ward, a microbiologist administered IV Ciprofloxacin and oral Linezolid (600 mg), which treats complex soft tissue infections. The microbiologist said to me that he would work with me for 6 months until ‘we found the right antibiotic.’
However, at the end of 48 hours, the consultant threw me off the ward. The ophthalmologist did not do a blood test before he discharged me to see if my neutrophils and ESR had normalised. He gave me one week’s worth of oral antibiotics. He then wrote to my then GP and told them to prescribe no more antibiotics. St. James’ Hospital and my then GP stopped all of my antibiotic medication. They did no blood tests first to check that my infection markers had normalised after the 48 hour IV treatment, before they did they terminated my medication..
Case To Answer
The consultant admitted me for 48 hours of IV antibiotics because of clinical evidence that I had an infection. Why on earth did the consultant not do a blood test to check that my neutrophils and WBC had normalised before he told my GP to stop my antibiotics?
York and Scarborough Teaching Hospitals

York Hospital
January 28th, 2014; Ophthalmology.
After St. James University Hospital kicked me off the ward, the consultant sent me to see his colleague, an ophthalmologist at York Hospital. I had one appointment at York Hospital. The consultant did no blood tests either to see if my infection markers had normalised following the 48-hour IV antibiotic treatment. He also wrote to my GP to order that my antibiotics be stopped. My treatment and care ceased in February 2014.
Spire Harpenden Hospital (Private)
5th Feb, 2014 – 12th March, 2014; Ophthalmology
I became very ill with nausea, chills, and a stiff neck after my then GP and hospital stopped my medication. The doors to NHS healthcare were closed in Yorkshire. I went to London to seek private medical help. Luckily, I found an oculoplastic surgeon at Spire, Harpenden. He was a lovely guy! He did a biopsy of my eyelid. My tissue histology came back chronically inflamed. The surgeon referred to me a professor of ophthalmology at St. Thomas’ Hospital, who specialised in inflammation of the eye. He also referred me to a physician at London Bridge Hospital. This surgeon thought that I had a systemic problem, which needed input from a physician. He thought this because my blood tests kept showing multiple abnormalities and raised markers.
HCA Healthcare (Private).

The London Lupus & Rheumatology Centre
2nd May, 2014- 2nd November, 2016; Rheumatology
I saw a physician at The London Lupus Centre for two years: 2nd May 2014–2nd November 2016. He was a fabulous guy, too! He was an intelligent physician who stabilised my condition. listened to me, and he believed me. On my first appointment with him, he did a series of blood tests. My neutrophils, WBC, haemoglobin count, and ESR were still raised. I had not had any medication since January 2014. That was five months! I remember shivering and throwing up in the flowerpot outside the hospital before my first appointment. I had awful chills washing up and down my left jaw area. The physician treated me empirically, with ongoing antibiotics, and monitored my bloods fortnightly. I felt much better systemically, but when I came off the antibiotics, my pain returned.
His opinion was that the infection had damaged my lymphatic drainage in my face, which is why the antibiotics only partially worked. He thought that I may have lymphoedema or angioedema. In 2015, the pain around my masseter/parotid area became severe. I could not open my mouth. The physician suspected that there was an obstruction in my parotid gland. He referred me to a well-known oral maxillofacial surgeon internally at London Bridge Hospital.
The Parliamentary Health Service Ombudsman

I tried to recover my treatment costs at London Bridge Hospital from Leeds Teaching Hospital and York Hospital, who stopped my treatment, but the PHSO did not uphold my complaint. The PHSO said I ‘chose to go to London.’ They ignored my MP’s statement, who I saw at the Houses of Parliament in February 2014. I went to him for help after St James’ Hospital kicked me off the ward. He phoned my then GP. The GP practice told my MP that they would refer me to another consultant if I found one in London and if they agreed with their diagnosis. I did not choose to go to London. The healthcare services had closed the doors to my medical treatment in Yorkshire.
London Bridge Hospital
July 2015 – 18th May, 2017; Oral Maxillofacial surgery
I saw a notable oral maxillofacial surgeon in July 2015 who agreed to see me on the NHS. He referred me to himself at the salivary gland unit at Guys Hospital for investigations of my parotid gland. He asked his clinic to do a sialogram to look for obstruction in my parotid gland. Guy’s Hospital is the national centre of excellence for salivary gland disease.
I saw him again after Guys Hospital prematurely discharged me. I saw him on 13/04/17, 20/04/17, and 18/05/17. There are serious questions about this surgeon’s transparency both in the NHS and privately.
Guy’s and St Thomas’ NHS Foundation Trust

Guy’s Hospital
27th January 2016 – 8th February 2017; Oral Maxillofacial surgery
27th January, 2016; I saw the surgeon, who I had consulted with at London Bridge Hospital in 2015. He did a sialogram, which showed obstruction in my salivary gland. They washed the obstruction away. He said at my consultation, ‘We found some obstruction, but it has all gone now.’ He discharged me, but he did not tell my referring physician at London Bridge Hospital that he found obstruction. The surgeon’s clinic letter from that date makes no mention of it.
I had relief of my symptoms for four days after this sialogram, but my symptoms returned after a week. My rheumatologist at London Bridge Hospital referred me back to see the oral maxillofacial surgeon, who I saw again privately. He referred me back to Guys’ Salivary Gland Unit on the NHS.
In June 2016, I had my second appointment at the salivary gland unit. Blood tests showed raised infection markers, neutrophils, and haemoglobin count. An ultrasound showed mucous plugging in my gland, a thickening of saliva. The consultant referred me for a sialendoscopy, which is an in-depth washout of my gland.
Sialendoscopies

In December 2016, a registrar did the sialendoscopy. When she entered the endoscope into my duct, we both saw on the screen big clumps of white at the top of my parotid duct. She said, ‘It is pretty clogged up in there. I am going to put you forward for washouts every six weeks.’ She referred me for regular washouts every six weeks.
On 31st January, 2017, I returned for another sialendoscopy with the lead dental radiologist and her assistant. They did an in-depth sialendoscopy and poured steroid drops down my parotid duct to treat the inflammation. I got huge relief from this procedure, but it was only temporary. I remember being so grateful for their treatment that I left a card for them at the clinic both saying, Thank you.
On 8th February, 2017, I saw the oral maxillofacial consultant one week later. She said that she was discharging me. She said that the lead dental radiologist, who had done the sialendoscopy, had reported that ‘everything was normal’ from the sialendoscopy in January 2017. It didn’t add up when the sialendoscopy from December 2016 had been abnormal, and the registrar who did that procedure had referred me for ongoing washouts every six weeks. Something wasn’t adding up. I suspected that the dental radiologist had not been honest about the clinical findings from my sialendoscopy.
My Complaint

July 2017: I complained to Guy’s & St. Thomas’ NHS Trusts about them promising me ongoing glandular washouts and then discharging me.
August 2017: The lead dental radiologist called me for another procedure. There were four registrars in the procedure room. During the ultrasound of my parotid gland, I heard the registrar say to the dental radiologist, ‘You are not freezing the images.’ It was at that consultation that the lead dental radiologist admitted to me that my parotid gland was not working properly, which revealed that she had not been honest about the clinical findings in January 2017.
If everything had been ‘normal’ with my parotid gland function in January 2017, why did the pathologist find an abnormality in my parotid gland tissue in 2018? (See incident 1 in the blog post; This is a Cover-Up). I do not believe that the lead dental radiologist was transparent about the clinical findings from January 2017.
St Thomas’ Hospital
30th June 2014 – 2nd November 2015; Ophthalmology
I had three appointments with a professor of ophthalmology at St. Thomas’ Hospital. This clinician diagnosed my left ptosis. He told me that the levitator on my left eyelid had collapsed and needed corrective surgery. The clinician said he couldn’t correct my ptosis until all of my symptoms had abated for six months. He said that the pain around my eye and cheek was a problem with the soft tissue. However, he did not act on that knowledge. He did nothing and discharged me when I still had severe periocular pain, saying, ‘I have not much to offer at this stage.’ He told my GP to refer me back for ptosis surgery once my symptoms had abated.
October 13th 2016; Infectious Diseases.
I saw an infectious diseases consultant once. He retested me for Lyme disease, which came back negative again. This consultant did other blood tests that showed raised infection markers and neutrophils, but he did not act on the findings. Instead, he said that I needed to see a ‘chronic fatigue specialist,’ which had no relevance to my facial pain symptoms or the haematology findings. I never saw him again. He was unpleasant with me.
Why?

Guy’s & St. Thomas’ NHS trust have a serious case to answer. All three departments—ophthalmology, oral maxillofacial surgery, and infectious diseases—found an abnormality, so why did they not deal with this back in 2016? Why did they all discharge me from their care? If my parotid gland was ‘normal’ in 2017, why did the histology from my parotid gland surgery show an abnormality one year later in 2018? It doesn’t add up.
Pennine Acute Hospitals NHS Trust

North Manchester General Hospital
6th September 2017 – 9th May, 2018; Oral Maxillofacial surgery
My then GP referred me to an oral maxillofacial surgeon at NMG, who I saw on 6th September, 2017. He agreed to do a superficial parotidectomy (the removal of the superficial lobe of my parotid gland), but he did not do a scan first. I signed a disclaimer before surgery to say that I may still have symptoms with my deep lobe after surgery. The surgeon said that he was not removing all of my parotid gland because of the risk of permanent facial nerve damage.
I also accepted the risk of facial nerve damage, which is common with parotid gland surgery because of the positioning of the seventh cranial nerve. The oral maxillofacial surgeon operated blind in April, 2018. I came through surgery with severe facial nerve palsy, which recovered in four months. The histology showed; dense secretions in the ducts, numerous calcifications, reactive lymph nodes. Parenchyma; sialolithiasis. The photos below show my facial nerve damage after surgery. I recovered full facial function in 4 months.



No Scan or Culture
The surgeon left me with a difficult predicament. A surgeon who I saw in Los Angeles confirmed in July 2019 that there was still 70% of my parotid gland remaining. The scan report from Los Angeles reported that some of the superficial lobe, the deep lobe, and some accessory tissue over the masseter muscle remain. The surgeon left a lot of my gland in! The surgeon did not cut and tie up the duct either. My parotid duct, which was thinned, was therefore still connected to the remaining portion of my parotid gland. I still experienced pain because of this. I did ask the surgeon why he did not cut and tie up my parotid duct. He said that ‘he couldn’t see it during surgery.’
Whilst I had a reduction of pain following surgery, because so much of the gland remained, I still had a lot of pain in the parotid area. I could not find a surgeon to remove the rest of it because of the risk of further facial paralysis. This was a tough predicament that the surgeon left me in. Another grievance is that the surgeon did not culture my parotid gland tissue. He knew that I had an infection in there because he diagnosed me with recurrent infections in the parotid gland. If he had cultured my tissue, we may have established what bacteria is causing this.

My discharge summary after my parotid surgery. Diagnosis: recurrent infections in parotid gland. Why did they not culture my tissue?
A Missed Opportunity
28th September, 2018; Infectious Diseases
I saw an infectious diseases consultant one time at The North Manchester General. This was a missed opportunity. This hospital had my parotid tissue in their laboratory. I asked the ID consultant if they would culture my tissue to find out what bacteria could be causing this problem. He refused. This is such a shame. If the hospital had cultured my parotid tissue, I could have found the potential bacteria that is responsible for my suspected infection.
He did not answer any of my questions about the ongoing antibiotics that I take. I wanted to know why the antibiotics relieved my symptoms in part when I took them, and then my symptoms returned when I came off them. However, he discharged me after one appointment with no offer of help or any answers. This guy could have done much more for me. He could have cultured my gland and tested me for Bartonella infection and other rare infectious diseases.
Case To Answer

If the surgeon had done a scan before he performed surgery, he would have seen that there was an abnormality in the entire parotid gland. If he was not confident enough to remove my entire salivary gland, he could have referred me to a surgeon who was. Why did he not do a scan first, and why did this NHS trust refuse to culture my parotid gland tissue? He knew that there was an infection in there, so why did he or his ID colleague not culture my tissue to find out what the bacteria was?
Sheffield Teaching Hospitals NHS Foundation Trust
Charles Clifford Dental Hospital
3rd Jan, 2019; Oral and Maxillofacial surgery Regional Unit.
I had one appointment regarding the pain in my remaining parotid gland. The surgeon examined my face and said that it is possible that there is some diseased glandular tissue left, causing the pain. He thought that my left masseter muscle was causing some of the problem, too. This consultant said that removing the rest of my parotid gland was too risky because of the potential risk of further facial paralysis. He prescribed hyoscine patches. You apply these to the skin, and they reduce salivary flow, but they were ineffective. He also told me to apply ibuprofen gel to the area where I am in pain. This was ineffective, also.
Lancashire Teaching Hospitals NHS Trust

Royal Preston Hospital
5th Feb, 2019; Oral Maxillofacial surgery
I had one appointment with a registrar, who could not help. He referred me on to an oral maxillofacial surgeon at Chorley Hospital.
Chorley and South Ribble District General Hospital
13th Feb, 2019; Oral Maxillofacial Surgery
This surgeon said he no longer does salivary gland surgery, and he referred me to another head and neck surgeon, internally at Chorley Hospital.
29th April, 2019; Ear Nose & Throat, Head & Neck services.
I had one appointment with a head & neck surgeon. He did no investigations and said that he could not remove the rest of my parotid gland because the risk of further facial paralysis was too high. He gave me no answers about any of my symptoms and referred me to Head and Neck Services at Manchester Royal Infirmary. I did not see the surgeon at Manchester Royal Infirmary until October 2019. It was a long wait to see him.
Imperial College Healthcare NHS Trust

Charing Cross Hospital on Fulham Palace Road.
Charing Cross Hospital
23rd May, 2019; Ear, Nose and Throat. Head and Neck services.
Something untoward definitely happened at Charing Cross Hospital. I saw a head and neck surgeon on 23rd May, 2019. He did four scans: MRI Neck, MRI Brain, CT Neck, and neck ultrasound. There was a serious gaslighting incident with this surgeon that I recount in incident 1 in Medical Gaslighting #1.
After I had had the four scans, I was in the surgeon’s office. I was sitting behind him, and he had all of my radiology images up on his screen. He enlarged one radiology image. There were huge white globules on the left side of my face. I politely asked the surgeon if that was calcified tissue. I asked him this because they found calcifications in my parotid tissue in 2018. He said ‘no’ and turned off his computer. ‘Your pain is psychological,’ he said. ‘You need to see a pain psychologist.’ His insolence and rudeness were impossible to tolerate, so I walked out.
My Missing Scan
I requested the four scans from Imperial College Healthcare Trust. I received the CD disc with my radiology images on it. When I opened the CD disc on my computer, I saw that there was no file icon next to the MRI neck scan. When I clicked on the MRI neck scan, an orange sign came up that said, ‘error decoding image.’ I looked through the other three scans, and I could not see the image that I saw on the surgeon’s screen of the white globules on my face.


I phoned the NHS trust and asked why the MRI neck scan had no file icon and was not there. They told me that they had merged the MRI brain and MRI neck scan images. I think they did do this, but I think that in the process of the ‘merging,’ they deleted some of the radiology images that showed abnormality. There was no reason to merge them like that. I am certain that if anyone conducted an audit trail of my radiology records from Charing Cross Hospital, they would find that they did delete some of my radiology images. This remains an unresolved issue. It needs investigating.
Liverpool University Hospitals NHS Foundation Trust

Aintree University Hospital
October, 2019; Head and Neck Services
My GP referred me to the oral maxillofacial department at Aintree Hospital. However, the department refused my GP’s referral without giving a reason why. I spoke to them on the phone, and they said, ‘There’s a lot going on behind the scenes that you don’t know about. We’ve been speaking to all of the surgeons who you have seen, and we don’t feel that there is a reason to review you.’ This is when I fell into a mental health crisis. The strain of trying to get medical help for my facial pain and being knocked back by NHS trusts like this was too much. This refused GP referral was the trigger for me falling into a mental health crisis.
Manchester University NHS Foundation Trust

Exterior Of Manchester Royal Infirmary Hospital
Manchester Royal Infirmary
11 May, 2018 – 29th June, 2018; Ophthalmology, Ocular plastic clinic
I saw an ocular plastic surgeon regarding my acute periocular pain two times. She gave me no diagnosis or treatment for my periocular pain. She discharged me after two appointments. They did give me some reading glasses for my blurred vision, which resulted from my post-surgery paralysis. She did refer back to The North Manchester General Hospital, to the Infectious Diseases department. It was this ophthalmologist who asked them to culture and do more tests on my parotid gland tissue, but ID at NMG refused.
25th September, 2018; Oral Maxillofacial surgery
I saw an oral maxillofacial surgeon regarding facial pain and post-surgery paralysis. He offered me no help regarding my facial pain, particularly the pain in my remaining parotid gland. He told me to go back to the salivary unit at Guys Hospital for a further sialogram because they ‘have the history on record.’
20th August 2019; Ear, Nose and Throat, Head and Neck services.
Following the referral from Chorley Hospital in April 2019, I saw a surgeon at Head and Neck services. He offered me Botox injections for my facial pain. I refused the Botox injections because with no diagnosis, we do not know what we are treating, and it could make my symptoms worse. I explain this in blog post; No to Botulinum Toxin.
After the obstacles I faced in England with consultants who were refusing to either see me or help me, I moved up to Scotland in January 2020 to see if I would have a better chance up there getting a resolution to my facial pain.
Fife Health and Social Care Partnership

Victoria Hospital
Nov 2020 – Jan 2021; Ear, Nose and Throat, Head and Neck services
I saw a head and neck surgeon for two appointments; once in November 2020 and once in January 2021. He did an MRI scan, which showed a left-sided enlarged masseter muscle. He referred me to head and neck tertiary services at NHS Lothian for specialist intervention.
November & December 2021; Infectious Diseases
I saw an Infectious Disease consultant. He did two blood tests in November and December 2021. They both showed abnormal/raised infection markers (neutrophils and WBC). He took no action and discharged me with abnormal blood results.
I asked the ID consultant if he would admit me for intravenous antibiotics, which I have been requesting for many years. He said no. He said in order for him to administer IV antibiotics, he would need Head and Neck services to remove the rest of my parotid gland and to culture the tissue. Once cultured, if they found the bacteria causing this, then he would administer IV antibiotics. He also said that when the surgeon removed my superficial lobe in 2018, they should have cultured the tissue to identify the bacteria causing this.
1st September, 2021; Pain Management
The surgeon, who I later saw at NHS Lothian (see below), referred me to the NHS Fife pain management service. The Fife Pain Management service refused to see me because ‘I was not suitable for their service.’ The question remains why pain management refused to even see me and why infectious diseases discharged me when they found raised infection markers.
NHS Lothian

The Royal Infirmary of Edinburgh
July-October 2021; Head and Neck Services, (ENT.)
My experience at NHS Lothian was the worst out of all the NHS trusts where I have been. This was absolutely horrific. It caused me enormous anxiety and distress. My experience at NHS Lothian was connected to what happened with the mental health services in Fife and a letter that a psychiatrist wrote, which said that I am making up my facial pain to feed the need ‘to have a sick role.’
I saw a head and neck surgeon in July 2020. I had one consultation with him. The surgeon said he would do some scans and get me back to ‘find a way forward.’ I had an MRI neck and CT neck scan in July 2020. I did not hear from the surgeon again. After I had the CT neck and bone scans done, he ghosted me for 18 weeks. I wrote to him three times asking for a follow-up consultation to explain the scans. He did not reply to any of my letters and did not discuss the scans with me. I have had outstanding questions about these images for 3 years. My visible facial asymmetry remains unexplained.


Duty of Candour?
The surgeon did refer me to Infectious Diseases in Fife, who discharged me after two appointments, and to Pain Management, who refused to see me. I complained to NHS Lothian about the fact the surgeon refused to give me a follow-up consultation. Their response was a terrible breach of the professional duty of candour. NHS Lothian said in their response to me that I needed to go to Fife Pain Management, but they knew that Fife Pain Management had refused to see me, as NHS Fife wrote back to the referring surgeon to tell them they had rejected his referral. NHS Lothian closed my case in October 2021 and left me with no care. They signposted me down a dead end, which they knew was a dead end.
The surgeon who I saw at NHS Lothian was the surgeon who made the discriminatory comment about me on the request form to the radiologist: ‘be careful with this one. Patient has significant psychiatric problems.’ Disgusting!

Case To Answer

Why did the consultant refuse me a follow-up consultation, and why did he ghost me for 18 weeks—why? Why did you give me no answers about the facial asymmetry in my CT scans, and why did no one catch the obscene comment that the surgeon made about me in his request to the radiologist? Someone in management should have caught that. Your treatment of me was appalling. Why? And why did you tell me in your response to my complaint to go to the NHS Fife Pain Management service when you knew they had refused to see me? Where was your duty of candour?
Ross Hall Hospital, Glasgow, (Private).

December, 2021; Oral Maxillofacial surgery.
Because the surgeon at NHS Lothian refused to see me for a follow-up consultation, I went to see an oral maxillofacial surgeon privately to get answers about the CT scan images that were done at NHS Lothian. I got no answers. There was a serious gaslighting incident with this surgeon, (see incident 2 in Medical Gaslighting #1.) He told me that my face was my spine in the radiology images below.


South Tees Hospitals NHS Foundation Trust
The James Cook University Hospital
April, 2022; Infectious Diseases.
I saw an infectious diseases consultant once. He did not answer my questions about why the oral antibiotics that I take subdue pain when I am on them, but why my pain returns when I come off them. He rudely said that the therapeutic effect that I get from the oral antibiotics was a ‘placebo effect.’ I took it to mean that he thought that I was imagining that the antibiotics helped me. I was not imagining anything. They do subdue my pain. The consultant said that he would only help if ENT thought that infection was the cause of my pain. He did no blood tests or investigations and discharged me after one appointment.
July, 2022; Oral Maxillofacial surgery
I saw an oral maxillofacial surgeon once. There was a serious gaslighting incident with this surgeon (incident 3 Medical Gaslighting #2). I asked him about my facial asymmetry in the CT scans that NHS Lothian did. He said, ‘Your head was lopsided in the scanner.’ He did not see me go into the scanner. I had the CT scans done in Scotland, and he was in Middlesbrough. Does he have X-ray vision from a distance? My face was not lopsided. I went into the scanner with my head in a head cage for God’s sake! He also rudely told me to ‘stop shopping around and live with the pain.’
Discharged Again!
The surgeon did agree to do an MRI scan of my brain and my parotid gland. Two weeks later, however, he wrote to me to say that he had cancelled the scans and discharged me. He said that oral maxillofacial surgery at York needed to deal with the problem because they found the abnormality on the scan (see below). I wrote to him to explain that oral maxillofacial surgery at York Hospital had refused my GP’s referral in April 2022, but he insisted that they had to see me.
November, 2022; Ear, Nose and Throat
I saw an ear, nose, and throat consultant (ENT) once regarding my left-sided ear pain. The consultant looked in my ear with an otoscope, said everything was ‘normal’ in my ear. He said I needed to see oral maxillofacial surgery at York Hospital. This clinician thought that my ear pain was referred pain from my parotid gland. He wrote to York Hospital. He discharged me after one appointment.
Nuffield York, (Private).
My Hospital Number; T30403626 Nuffield.
June 2022; Ear, Nose and Throat, Head and Neck Services.
I saw a head and neck surgeon, who looked at CT scans that NHS Lothian did. He said that he ‘could definitely see the asymmetry in my face,’ and that he wanted to ‘get to the bottom of what was causing my facial pain.’ He agreed to see me on the NHS at York Hospital to do further imaging so that he could compare new scans to the ones that NHS Lothian did in 2020.
York and Scarborough Teaching Hospital
York Hospital
July 2022 – September 2022; Ear, Nose and Throat, Head and Neck.
I saw the head and neck surgeon, who I had consulted with privately at Nuffield York in July 2022. The surgeon sent me for an MRI neck scan and a head CT scan. One month later, he wrote to say that the MRI scan had shown an abnormality in the left buccal fat pad area. He said that the oral maxillofacial surgery team needed to deal with it, not ENT.

However, the oral maxillofacial team at York Hospital refused my GP’s referral in April 2022 because my ‘case was too complex.’ The ENT surgeon sent my case up to James Cook Hospital. James Cook Hospital sent it back to him and said it needed to be dealt with at York Hospital because they found the abnormality. My case was passed back and forth between York Hospital and James Cook Hospital. Neither hospital wanted to deal with it. It was a game of tennis.

I saw the same ENT consultant again on 15th September, 2022, regarding the pain that I have had around the left side of my head and in my left ear.
However, he refused to help me. The consultant said that the oral maxillofacial surgery team needed to deal with it because the problem involves my temporal region. He thought that my head and ear pain was pain that was referred from the parotid/buccal area. My GP wrote to him again about my worsening head pain. The surgeon replied to my GP and told him to refer me to a skull-based otolaryngologist at Leeds Hospital. This surgeon abdicated from taking any responsibility for the abnormality that he found. He should have dealt with it.
York Hospital, Ophthalmology

October, 2022; Ophthalmology
I saw an ophthalmologist regarding my eye pain. It was strange returning to the department as I saw this team in 2014, after St James’ Teaching Hospital kicked me off the ward. They still had my notes from this time, though the consultant who I saw this time was a different guy from the one who I consulted with in 2014.
The consultant was shocked to see me again. He was defensive and would not answer any of my questions about the scans. When I showed him the radiology images of my left eye, he dismissed it as being the ‘angle of the scan.’ He did, however, say something poignant about my eye pain. He said, ‘The issue is with the tissue.’ This indicated that he knew I had a problem with the soft tissue around my left eye. He gave me no answers, help, or treatment. He did say that the abnormality found in my buccal fat pad area needed to be followed up, and he wrote to oral maxillofacial surgery to ask them to see me.

Medical Gaslighting
April 2022 & February 23rd, 2023; Oral Maxillofacial surgery
Oral maxillofacial surgery at York hospital finally agreed to see me, having rejected my GP’s referral in April 2022. My appointment with him was on February 23rd, 2023. This appointment was horrific. A serious gaslighting incident occurred, (see incident 4 in; Medical Gaslighting #2.)
I asked the surgeon about the abnormality that they found from my MRI scan. He told me that the abnormality that they found was caused by a tooth of mine. It was not to do with a tooth. I showed the surgeon my MRI radiology images that I had on my iPad. I asked him to explain them. ‘That’s just coincidence. You are choosing to see it,’ he said. The surgeon said that to me about the radiology images below.


He brought my radiology images up on his screen. He started to Photoshop the images so that you couldn’t see the abnormality anymore. ‘Look, the abnormality has gone,’ he said. He then proceeded to Photoshop the images again, so that the abnormality showed on my right side. ‘Look, I can make it show on your right side. It’s just the angle of the scan.’ It was like sitting next to Paul Daniels, not a surgeon. I showed him the CT images from NHS Lothian on my iPad and asked him about my facial asymmetry in the images. ‘The quality of your iPad is s**t,’ he said. The surgeon said that about the radiology images below.


Case To Answer
He proceeded to tell me that all of my CT images are ‘squint images.’ He told me that my MRI images were ‘coronal view and that the scans were not accurate. This made no sense. I tried to question him. ‘The data is still here,’ he said. He had sheepish eyes when he said this. I did not return to see this surgeon for the follow-up appointment that he arranged. Two hours with him playing ‘now you see it, now you don’t’ was too distressing. The experience messed with my head. I came out of the appointment distressed and questioning my own sanity.
No one at York Hospital explained the abnormal MRI neck scan that they found in July 2022. I have been to three departments there: ophthalmology, ENT, and oral maxillofacial surgery. The main issue is why they sent my abnormal scan up to James Cook Hospital to deal with instead of dealing with it themselves. When York Hospital finally allowed me to see an oral maxillofacial surgeon, he gaslighted me and told me that I was imagining the abnormality. They found an abnormality on my MRI scan in July 2022. Why did they not explain to me what it was and act on it right away?
The End Of The Road

It was after the last appointment with oral maxillofacial surgery at York Hospital on 23rd February, 2023, that I decided to walk away from any further consultations. The abuse and bullying from these consultants were putting my mental health in too great a jeopardy. I wrote to the practice manager at my GP practice and explained that because of the impact these consultations were having on my mental health, I would not be attending the follow-up appointments at York Hospital with oral maxillofacial and ophthalmology.
I decided to stop attending appointments with medical consultants and to write my blog and network on social media, to try and find medical help that way instead.
Leeds Teaching Hospital NHS Trust

Leeds Dental Institute
24th June, 2022; Oral Maxillofacial surgery
Refused GP Referral: No Reason Given
After oral maxillofacial surgery at York Hospital refused my GP’s referral in April 2022, they told my GP to reroute the referral to a named specialist at Leeds Teaching Hospital. My GP sent the referral to Leeds Teaching Hospital, but they discharged me without seeing me. They refused to give me an appointment. They closed my case down and did not even send a letter to my GP, informing him of the rejected referral. I found out when I phoned them.
Mental Health Trusts

South West Yorkshire Mental Health Trust
Oct 2019- Jan 2020; Crisis Team
Due to the strain of all this, I fell into a serious mental health crisis in October, 2019, when I began to experience chronic suicidal ideation. I was under the care of the crisis team at South West Yorkshire Foundation NHS Trust from October 2019 to January 2020. I have documented the incidents that occurred with this mental health trust in my previous blog post: On mental health crisis #2. Their treatment of me was punitive.
The Letter!
Fife Health and Social Care Partnership
Feb 2020- Feb 2021

I arrived in Fife in crisis. The events with the NHS trusts in England, who had failed to treat my facial pain, were the trigger and cause of my mental health crisis. My GP referred me to the mental health team in Fife. They admitted me for ‘respite’ to Whyteman’s Brae inpatient unit for two weeks in February 2020. After I was discharged, I was under the care of a sweet mental health nurse, who phoned me weekly to help me with my distress about what was happening regarding my facial pain with the medical profession.
In January, 2021, I withdrew from the mental services in Fife because of a serious incident with a psychiatrist who I had never met. It was horrific. This man had never met or spoken to me, and he wrote a dangerous letter about me, which negatively impacted the way head and neck surgeons viewed me. His letter said that I have ‘factitious disorder’ and am making my facial pain up. The letter that he wrote was the reason behind the discriminatory treatment from the surgeon at NHS Lothian. I did not want mental health services to write any further letters of this nature about me, so I felt that I had to withdraw from their care.
I raised a complaint about the psychiatrist with the General Medical Council.
TW: This section of the post contains wording about suicide that some readers may find triggering. If you are in the UK and your need is urgent, please call 999. If you need support, please call 111, option 2, or Samaritans freephone; 116123.
Tees Esk and Wear Valleys NHS Foundation Trust

Princess Road Clinic, Malton
Feb 2022 – 2nd May 2024
I have documented all of the incidents that occurred with Tees Esk and Wear Valleys NHS trust in my next blog post. In summary, they told me that I needed to ‘reframe’ the way I look at what has happened with the NHS and my facial pain. In May, 2024, they prematurely discharged me when I was still actively suicidal. A psychiatric liaison officer who I saw at Scarborough Hospital in June 2024 told me that I could not return to A&E for mental health support again. He told me that I had to find help ‘in the community.’
I saw a psychiatric liaison officer at York hospital A&E in August 2017 who referred me back to the CMHT. The CMHT still refused to give me any support or signpost me anywhere even when psychiatric liaison team from A&E had referred me back to them for support. The CMHT prescribed me a repeat dose of Zopiclone to help with my chronic insomnia. However, they did not offer me a review to see how I was responding to the medication. They discharged me again in December, 2024. This is extremely dangerous to prescribe a sleeping tablet and not review a patient.
TEWV Crisis Team

My experience with the crisis team at Tees Esk and Wear Valleys NHS Trust (TEWV) has been heart-breaking. The psychiatric liaison team at Scarborough Hospital first referred me to them in April 2022. The first period of their involvement was positive. They hurried through a referral to my CMHT for urgent mental health support. They also referred me to the adult social care department at North Yorkshire County Council for a support time recovery worker. My GP referred me back to them a year later. They visited me at home once and told me to ‘distract myself.’
Betrayal and Dishonesty
The third time has been devastating. Following a suicide attempt that I made on 7/02/25, Northumbria Healthcare NHS Foundation Trust, which treated me with IV NAC, contacted the crisis team at TEWV and told them that I required an informal admission onto a psychiatric ward in Yorkshire because I was still at risk. Northumbria Healthcare NHS Foundation trust told me that the crisis team at TEWV were arranging an informal admission for me onto a ward at Cross Lane Hospital in Scarborough. They told me that TEWV would call me to clarify the details. The discharge summary from Northumbria NHS Foundation Trust states, ‘Felicia has been offered an informal admission to a psychiatric ward in her own locality (York, Yorkshire) due to risks identified.’ It also states that Northumbria psychiatric liaison team and crisis team have no more responsibility for my care.


However, on 9/02/25, after Northumbria NHS Trust had discharged me, the TEWV crisis team told me on the phone that there ‘were no beds in Scarborough’ and that they ‘didn’t agree to an informal admission.’ They told me that Northumbria NHS Trust had miscommunicated this to me. I explained to them that my discharge summary stated that they were arranging an informal admission, but they insisted they were not doing so and that they ‘were sorry to disappoint me.’
I told them that I still felt suicidal, and they told me to go back to the A&E where they treated me for my overdose. They were playing a game of table tennis with my life. When would they stop playing games with my life? I don’t know what happened in the correspondence between these two NHS trusts. They had not been truthful with me. The fact that they had lied to me after a suicide attempt was devastating.
6 Appointments

The TEWV crisis team gave me six outpatient appointments at Cross Lane Hospital, Scarborough. There was no admission. The first nurse who I saw told me that they were not admitting me. She said that Northumbria NHS had phoned them and told them that I didn’t need a bed anymore. More lies. I have a recording of the crisis team in Northumbria saying that I needed an admission onto a ward. These lies were confusing and hurtful. I had woken up to more duplicity than I had gone to sleep with.
The same nurse asked me at my second appointment if I still had plans to end my life. I told her that I did. She asked me what they were. I disclosed my suicide plan to her. She said, ‘You need to keep your cards close to your chest; otherwise, your plans will be scuppered again.’ I was stunned. I could not believe what I was hearing and that I was sitting opposite a mental health nurse. My interpretation of this was her saying, ‘Go commit suicide, but keep quiet about it so your plan will succeed.’
I had two appointments with the psychiatrist on the crisis team. He said, ‘We need to get this chronic facial pain sorted.’ At last! I thought someone was going to intervene. He committed to getting my medical records and speaking to the medical consultants about what was happening with my facial pain. But it was false promises. All he did was phone my GP and ask him to refer me to another specialist—the 19th NHS trust. His actions showed cowardice. I wanted him to fulfil on his promise and speak to the clinicians themselves, but he didn’t. He backed down.
Discharged
The crisis team have discharged me after 6 appointments and left me with no mental health support 3 weeks after a serious attempt to end my life. My CMHT continue to refuse to see me or offer any support and they have not signposted me anywhere. I feel mistreated and let down by the crisis team at Tees Esk and Wear Valleys NHS Trust, and by the NHS trust as a whole. To be left with no mental health support after a genuine attempt to end my life is devastating and frightening.
Lastly, following my suicide attempt, I posted on X (formerly Twitter) about the dishonesty regrading the mental health bed that I was promised that did not exist. The Care Quality Commission (CQC) saw my post and kindly asked North Yorkshire County Council (NYCC) to safeguard me. A member from the crisis team told NYCC that I did not need safeguarding. This led to NYCC closing down the CQC’s safeguarding request and taking no action on the concern. NYCC have put no safeguarding in place. This has left me with no support and no safeguarding.
Case To Answer

It is indisputable that all three mental health have trusts failed me.
What has hurt so deeply is how 3 mental health trusts and 3 crisis teams remained quiet. They all know that I am not making my facial pain up, so I have struggled to understand why they did not pick up the phone and speak to the medical teams about the impact that the pain was having on my mental health. The conduct of Tees Esk and Wear Valleys NHS Trust needs accounting for. They need to account for why they discharged me when I was struggling with suicidal ideation. They also need to account for why their psychiatric liaison officer told me on June 10, 2024, that I could not return to A&E for mental health support again.
Last but not least, this NHS trust needs to answer why Princess Road Clinic, Malton, refused to offer me any help when one of their psychiatric liaison officers at York hospital A&E referred me back to them in August 2024. There is an internal contradiction here. The CMHT needs to also explain why they prescribed me Zopiclone on repeat and offered me no follow-up about this medication. This is dangerous.
Why did you tell Northumbria NHS Trust that you were arranging an informal admission for me onto a ward in Scarborough when you clearly had no intention to do so? Where was your duty of care? Why lie to me when I was at my most vulnerable? What do you expect me to do now? I am still suffering with suicidal thoughts, and I have no mental health support. The crisis team has discharged me. My CMHT still has no intention of offering me any support, and two of your liaison officers at both York and Scarborough hospitals have told me that I cannot go to A&E again to receive help with my suicidal feelings. What do you expect me to do?
Why on earth did you tell NYCC to not put any safeguarding in place?
Northumbria Healthcare NHS Foundation Trust
Northumbria Emergency Specialist Care Hospital,
7/02/25-9/02/25
I made an attempt to end my life on 7/02/25, which I speak about in a separate blog post that I will be publishing shortly. I took a mixed overdose near Alnmouth beach in Northumbria. As I understand it, I passed out shortly after I took the overdose, and two groundsmen from the golf course found me and called an ambulance. I have no memory of any of it, only that I woke up at 10.00pm at Accident and Emergency.
The clinical team was outstanding at Cramlington emergency specialist care hospital. The medical team administered IV NAC for twelve hours. They told me that it was successful because they got to me quick enough from the time of the ingestion. I can only praise their care while I was on the ward from 7/01/25 to 9/02/25.
Psychiatric Liaison Team
Sadly, the care from the psychiatric liaison and crisis team at this Northumbria Healthcare NHS Foundation Trust did not match the clinical care that I received on the ward. They left me in a highly vulnerable predicament. After I woke up, I made it overtly clear to the clinician who administered the IV NAC that I was still suicidal. The clinician promised me that they would not discharge me without mental health support. I asked both the psychiatric liaison team and the crisis team if I could see a psychiatrist. They both said no. I asked them if I could have a short-term admission onto a bed on a mental health ward in Northumbria until I felt I could keep myself safe. I told them that I would prefer to be admitted into a unit in Northumbria because Tees Esk and Wear Valleys NHS Trust had discharged me.
CNTW Crisis Team

Following an assessment, Cumbria, Northumberland, Tyne and Wear NHS Trust (CNTW) crisis team concluded that I was still at risk and that I needed an informal admission onto a psychiatric ward. They told me that the bed manager at Tees Esk and Wear Valleys NHS Trust was arranging an informal admission for me onto a ward in Scarborough. I asked them to confirm where this bed was and when it would be available. They said they could not confirm the details and that the TEWV crisis team would be in touch.
My discharge summary clearly states, ‘Felicia has been offered an informal admission to a psychiatric ward in her own locality (York, Yorkshire). It also states that there is ‘no further role for the psychiatric liaison team or crisis team in Northumberland.’ However, the TEWV crisis team told me on the phone that there ‘were no beds available in Scarborough’ and that they never promised me an informal admission. TEWV said that Northumbria NHS had miscommunicated this to me. It appears Northumbria NHS Trust had not been honest with me about this.
Unsafe Discharge

Despite the exceptional clinical care that Northumbria NHS Trust provided during my time on the ward, the NHS trust misled me. They told me that the crisis team at TEWV was arranging a bed for me in Scarborough that did not exist. They also blocked me from the crisis team and said they had no more responsibility for my care. This meant that I could not go back to them for any help to resolve the issue with TEWV. Additionally, when I left the ward, the ward sister handed me back the carrier bag with the remaining whisky and paracetamol tablets that I used to try and end my life.
This was not a safe or careful discharge.
Case To Answer

It was the systemic coldness, the lack of transparency, and the abdication of responsibility for my care by multiple NHS trusts that pushed me to try and end my life. You continued to treat me with the same coldness and dishonesty after my suicide attempt.
You identified that I was still at risk, so why didn’t you therefore ensure that I had a bed on a psychiatric unit before you discharged me? That would have been a safe way to discharge me instead of throwing me out into the wild with no support. Why did you hand me back the bag with the remaining whiskey and paracetamol tablets in it that I had used to try and end my life when you discharged me? Throw them away next time.
My Current GP:
Ampleforth Surgery, March 2022-present.
There have been six other GP practices involved in this case from 2013.
North Yorkshire County Council

Adult Social Care
The General Medical Council’s Victim Support Service referred me to North Yorkshire County Council, (NYCC) for safeguarding in February 2022, before I moved back to England. I have documented the incidents that occurred with this local authority in my blog post, On Suicide.
In summary: In March, 2022, a social worker assessed me as meeting the threshold to receive statutory social care support. She assigned me a support time recovery worker and agreed with me that when I moved to a place that was more central, where support agencies could come to me, my direct payments would be instated. In April 2023, a new social worker took over my case. She came to my house and told me they were stopping my support and closing my file. They did this without reassessing me, which is a breach of the Care Act, 2014. NYCC ignored the advice of my GP, who asked them to continue my support, and the clinical advice of a psychiatric liaison officer, who wrote to NYCC in March 2023, explaining that withdrawing my support would put me at risk.
I complained to the chief executive of North Yorkshire County Council . I never got a response from him or anyone at the council. The police referred me back to NYCC a year later, but my local authority closed my file again. Following my recent suicide attempt on 7/02/25, the Care Quality Commission (CQC) asked NYCC to safeguard me. NYCC have closed down the CQC’s request and have taken no action. They have not safeguarded me.
Conclusion

All of the NHS trusts that are listed here have a case to answer to about my care over the last 12 years. There have been serious failings with most, if not all, of the trusts. Many of the consultants and GPs who I have seen have deviated from Good medical practice. They have not listened to me; they have not answered my questions. Many of the clinicians who I have seen have overlooked clinical findings or not been honest about abnormalities they have found. If they have been honest about what they have found, then they have failed to act on those findings. All of this combined has forced me to endure unnecessary amounts of pain and suffering for what will be 12 years this May, 2024. The key areas where these NHS trusts failed in my care are:
- Delayed Diagnosis and medical treatment/intervention
- Lack of continuity of care
- Lack of advocacy
- Lack of transparency and Accountability.
- Refusal to answer my questions about my condition.
Pathology Found:


- Abnormal blood tests; continuous raised neutrophils, infection markers, haemoglobin count and MCHC.
- Left ptosis; collapsed levitator
- Malfunctioning parotid gland; mucous plugging.
- Hardened/calcified parotid gland tissue.
- Sialolithiasis
- Reactive lymph nodes
- Enlarged masseter muscle
- Unexplained abnormality in buccal fat pad/ retromolar area
The pathology that you all found points to an infection as the likely cause of my condition, so why did you refuse to acknowledge this for so long? I struggle to understand why four infectious disease consultants at NHS Fife, James Cooke Hospital, St Thomas’s Hospital, and The North Manchester General Hospital refused to try intravenous antibiotics. I asked all four consultants, repeatedly, why the antibiotics that I took for 11 years abated my symptoms when I was on them, but then my symptoms returned when I came off them. None of them gave me an answer.
All four clinicians ignored blood tests that showed raised neutrophils, WBC, and other abnormalities. They took no action. Surely, IV antibiotics would have been better than doing nothing?
The case to be answered by all of these NHS trusts who have been involved in my case, is why they have overlooked the pathology that they found and haven’t put it together to come up with a diagnosis.
If it isn’t an infection, then what the hell is it?

Foot Notes
[1] Guidance: The Public Interest Disclosure Act, www.gov.uk
Photo Credits: Karl Moran, Angelo Abear, Jeremy Mcgilvrey, Neil Martin and Andrew Hall on Unsplash. Ekaterina Bolovtsova, Janson A, Ann H, Anna Tarazevich, Shvetsa, Roberto Carrafa, Mart Production, PNW Prod, Cottonbro studio, Krivitskiy, XPlore Heritage, Wojtek Paczes, Howard Senton, Ekaterina Bolovtsova and John on Pexels. Pirkko Seitsenpiste, Gerd Altmann and Markus Winkler on Pixabay.

2024-12-18 06:03
On Mental Health Crisis #2
Mental health crisis #2 openly discusses the topic of crisis. There are also references to suicide that some readers may find triggering. If you are in the UK and your need is urgent, please call 999. If you need support, please call 111, option 2, or Samaritans freephone number, 116123.
Introduction
‘Like any other health crisis, it’s important to address a mental health crisis quickly and effectively. Crises can be difficult to predict because, often, there are no warning signs.’[1]
This post follows on from my previous post. In that post, I discuss my five-year-long mental health crisis that has arisen because of living with undiagnosed facial pain for so long. This post discusses the dismal response that I have received from the mental health services. I will be recounting my experience with the two most recent community mental health teams (CMHTs) and my experiences with two crisis teams.

This post also raises the question as to why statutory mental health services fail so many patients. It calls out for the English government to pour more money into non-statutory support services in order to provide a safety net for vulnerable patients, who, like me, have been left with no support.
CMHT 1: Fife

My experience of the mental health services in Fife was unjust and devastating. I moved to Scotland in January 2020. The motivation behind my move to Fife was to look for medical help for my facial pain. Naively, I thought that I might get a better response from the medical teams across the border.
I arrived in Fife five months into my mental health crisis. I have already blogged about how a psychiatrist in Fife, who had never met me or spoken to me—I didn’t even know who he was—went into my records and wrote a discriminatory letter about me in December 2020. His letter said that I have “factitious disorder” and that I am making up my facial pain to feed the “need to have a sick role.” He sent that letter to multiple agencies.

In Scotland, they have a medical recording system called Sci Gateway. Any medical professional across all of Scotland has access to a collective database of your medical records. The head and neck surgeons who my GP had referred me to could see the psychiatrist’s letter. His letter thwarted my whole reason for moving to Scotland: to get medical help for my facial pain. Two head and neck surgeons stonewalled me after he published his letter. His letter also led to systemic mental health discrimination, which I fell victim to.
This incident was a cruel injustice. A mental health professional who I had never heard of completely thwarted my chances of being taken seriously by the medical teams and getting medical treatment for my facial pain. I fell into a more serious mental health crisis after this.
CMHT 2: North Yorkshire

I didn’t think anything could be more unjust than my experience with the mental health team in Fife, but my experience with the mental health team in North Yorkshire has been even worse. My CMHT colluded in an underhanded manner with the cover-up about my facial pain. They then put the responsibility for their complicity onto my shoulders.
I arrived back in Yorkshire from Fife in February 2022. I was still in crisis. Even when the CMHT in North Yorkshire accepted me onto their caseload, they only saw me once every three months, (if I was lucky). On more than six occasions, I turned up for an appointment, and the MH clinician wasn’t even there. When I was actually seen, the “mental health nurse” told me that I need to “reframe” the way I view everything, that I “don’t like what I’m hearing from surgeons,” and that I need to hear some “hard truths.” She never specified what those “hard truths” were.
The Psychiatrist

I only saw the lead psychiatrist of my MH team twice in two years. I confided in the psychiatrist and told him that I had seen on my medical records that my GP had written: scan abnormal, to be expected, no further action. Within two hours of telling him this, I could not log into my TPP System One account. My GP practice had locked me out. When I got a new password, I saw that the GP practice had amended that comment. They had added: no review applicable to that record.

The underlined wording in red is the amendment that the GP practice made to the record 18 months after it was initially made.
It was the psychiatrist’s sneakiness that I found so sinister. He must have called the GP practice within minutes of me leaving the clinic. But I clocked him. I saw through his sneaky.

The psychiatrist could have helped me. He could have questioned my GP about why they had ignored an abnormal MRI scan. He chose instead to protect the GP. This is how the cover-up culture works. It’s one thing to be complicit in the falsifying of my medical records. It’s a whole other thing to then put the responsibility onto my shoulders: to tell me to “reframe” it. Cruel doesn’t touch the sides. It’s corruption at its worst.
After my CMHT discharged me, I went to A&E on May 17th 2024 to get help with my suicidal feelings. My GP practice then deleted that visit to A&E from my medical records. On 10th June, 2024, when I back to A&E, the psychiatric liaison officer told me that I could not go back to A&E for support again. They told me self-refer back to agencies who they knew had closed my file.


In their discharge letter, the CMHT said, ‘Felicia thinks that NHS bodies are colluding with each other.’ The psychiatrist giving my GP practice the heads up to amend my medical record was colluding with them. When my GP practice deleted from my record that I went to A&E for suicidal feelings on May 17th, it was to cover for the CMHT, who they knew should not have discharged me. If this isn’t colluding with one another, then what is it?
Shut Down Again

In August, 2024, I went to A&E for the third time this summer to get help with my suicidal feelings. I saw a psychiatric liaison who referred me back to the CMHT. The CMHT did another assessment in November 2024 but said that they cannot provide me with any help or signpost me to other support agencies. I asked them what I should do regarding coping with my suicidal feelings.
‘Your suicidal ideation is chronic, but we can’t help,’ they said. ‘It’s your facial pain that is causing your mental distress, so your facial pain needs sorting. That’s not our responsibility, I’m afraid.’ I felt sickened and angry that she downplayed my struggle with suicidal ideation while smirking.
Any talk of suicide should always be taken seriously. Most people who attempt suicide have given some warning—but this isn’t always the case. If someone has attempted suicide before, the risk is even greater.
Crisis Teams
‘Crisis resolution and home treatment (CRHT) teams were introduced in England from 2000/01 with a view to providing intensive home-based care for individuals in crisis as an alternative to hospital treatment.’ [2] They act as gatekeepers within the mental healthcare pathway, and are supposed tom allow for a reduction in in-patient admissions. They are also supposed to reduce out-of-area treatments and support earlier discharge.
Jacobs and Barrenho conducted a study to investigate whether the introduction of crisis teams and home-based intensive treatment teams actually reduced the number of in-patient hospital admissions. They found no evidence that crisis resolution and home treatment policy have made any difference to inpatient admissions. They rightly state that there is ‘a need for more research on the policy as a whole.’[3]
I am not surprised by their conclusion. I have been under the care of two different crisis teams during my mental health crisis, and my experience has been appalling. One team caused me harm, and the other tried to pass the buck back to the CMHT. An inpatient hospital admission would have been much more helpful.
Crisis Team 1

My first contact with a crisis team was in West Yorkshire in 2019, when my mental health crisis began. When I first fell into a crisis in 2019, I did make a suicide attempt. I spent three nights at a hospital in Kent after my attempt. My local crisis team assured the psychiatric liaison team in Kent that they would give me a bed on my local ward in West Yorkshire on my return. The hospital in Kent sent me back home in an ambulance. When I arrived back, the crisis team in West Yorkshire told me that there was no bed.
They then sent the police to kick down my door as part of a ‘welfare check.’ I returned home at midnight to find that the police had boarded up my door. I phoned my crisis team and told them that I could not gain entry to my home. Their response was criminal. The lady who answered the phone said, ‘You’ll have to sleep rough. That’s consequences for your actions. You shouldn’t have done it.’
It felt like persecution.

Crisis Team 2

The response that I have had from the crisis team in North Yorkshire has been equally poor. They visited me at home for three days in 2022. I had just arrived in North Yorkshire, having been living in Fife. They referred me back to the CMHT. My GP was concerned about my welfare and referred me back to the crisis team in 2023. They visited me at home again. This time, they told me to ‘distract myself,’ but it’s challenging to distract yourself when you are in a suicidal crisis.
The crisis and home-based intervention teams decide whether or not to admit a patient onto a psychiatric ward. They do whatever they can to refrain from this. However, if a patient is in the throes of a mental health crisis, an inpatient admission is often the best thing. The 24/7 support provides a safety net that patients need when they are in crisis. In my experience, the crisis and home-based intervention teams do not offer this safety.
Signposting

A common action that mental health services take when they decline to help a patient is to ‘signpost’ them to non-statutory services. Non-statutory services refer to local charities that offer mental health support in the community and national helplines like Samaritans and Campaign Against Living Miserably (Calm). Community mental health teams sometimes signpost people to the local authority. ‘Where support is not available under The Care Act, local authorities provide information about non-eligible needs.’[4]
The reality is that most areas in England have few third-sector agencies that provide support in the community. In North Yorkshire, there is one charity in Scarborough that provides support. The only other non-statutory service is Supporting Victims which provides counselling support to people who have been victims of crime. That’s it.
There are many more third-sector agencies that provide mental health support in Scotland. SAMH, Breathing Space, and Housing Support are just a few to name. The Scottish government pumps a lot more money than the English government does into funding non-statutory services. I was extremely impressed by the third sector in Scotland.
Non-Statutory Support
If a CMHT declines to help a patient who is in a mental health crisis and ‘signposts’ them to the community, and there are no alternative agencies who can help, the vulnerable patient is left with no support. This puts a vulnerable patient at risk.
I have been ‘signposted’ back to my local authority, who refused to help me. The CMHT also gave me a number for the crisis team, but I can never get through to them. They have left me with no support. There are not enough charities in England to pick up the slack from CMHTs, bar a few national helplines, bar a few national helplines. If community mental health teams continue to ‘signpost’ instead of helping mental health patients, then there must be non-statutory support available. It’s not fair to signpost patients to community services that don’t exist. It’s like leading someone to a swimming pool with no water.

Conclusion
I am not alone in my experiences of the mental health system. My feed on X (formerly Twitter) is full of posts from people whom mental health services have failed. I read so many posts from patients who are in need of help and support but whom the MH services have dismissed. One lady recently posted about how her crisis team hung up on her when she rang them for support.
In 2020, Sir Simon Stevens, the previous chief executive of NHS England, said, ‘The NHS is delivering on its pledge to improve mental health support.’[5] The NHS is not delivering on the pledge. The mental health system fails too many of us. The gap between these words on paper and the reality for patients like me is too big. It needs bridging. Health executives need to put these words into action.
But, why are services that mental health teams provide generically so poor? Is it because they do not have the resources to meet the heavy demand on services? Or is it due to a lack of compassion and empathy? I don’t know. However, if statutory mental health services continue to fail so many patients, then the English government must pour more funding into the third sector/non-statutory services to ensure that there is a safety net for patients.

I feel abandoned and trodden on by the mental health services. At the very least, the mental health services could have communicated to the medical teams about how badly my facial pain is affecting my mental health. They have not advocated for me at all. They have remained silent, which is a form of complicity. The word that best describes the response from mental health services to my mental health crisis is betrayal. And it’s hurt.

A Tribute
I want to extend a heartfelt thanks to all of the non-statutory organisations that have helped me weather this storm. I have been heartened and touched by their kindness. It’s thanks to you all that I have made it this far. All of the charities mentioned in this post that have a hyperlink are charities that have supported me during my five-year-long mental health crisis.
I don’t think that charities get enough recognition for the extraordinary work that they do in communities around the UK. I have experienced nothing other than dedication, kindness, and integrity from every worker and volunteer I have come into contact with. You are my heroes and heroines, and on behalf of myself and the thousands of others whom you help, a massive thank you.

Foot Notes
[1] The National Alliance on Mental Illness, (NAMI), Navigating a Mental Health Crisis
[2] Jacobs R & Barrenho E: The Impact of Crisis Resolution and Home Treatment Teams on Psychiatric Admissions in England. Feb, 2011, The British Journal of Psychiatry: the journal of mental science.
[3] This quotation is taken from the same source as footnote 2.
[4] Care Quality Commission: The State of Health Care and Adult Social Care in England, 2023/24, www.cqc.org.uk
[5] NHS England: Mental Health Crisis Services Rolled Out Across England, March 2020, www.england.nhs.uk
Photo Credits: Prawny on Pixabay. Alexsi Partanen, Jose P Ortiz, Burkhard Kaufhold, Jametlene Reskp and Masaaki Komori on Unsplash. Tima Miroshnichenko, Tom Gill, Timur Weber, Pavel Danilyuk, Julia Cameron, Olha Ruskyth, Jeff Stapleton, Brett Sayles, CK Lacandazo and Mart Production on Pexels.

2024-12-02 05:12
On Mental Health Crisis #1
Mental health crisis #1 openly discusses the topic of distress and crisis that some readers may find triggering. If you are in the UK and your need is urgent, please call 999. If you need support, please call 111, option 2, or Samaritans freephone number, 116123.
Introduction
‘A mental health crisis is when a person’s emotional or mental state puts them in danger or prevents them from being able to care from themselves or function effectively in the community.’[1] ‘Crisis occurs when something happens or a series of events happen that take you over the edge and reduce your ability to cope or function normally. Stress and sudden changes in your personal life such as the death of a loved one, divorce, the loss of a job, incarceration or illness can all result in emotional overload and overwhelming feelings of helplessness.’[2]
Very Well Mind describes a mental health crisis as ‘when you are so overwhelmed with emotions like fear that your go-go coping mechanisms aren’t helping. Being in a state of crisis means that you’re so afraid and confused that you can’t make decisions.’ Mental health crisis #1 discusses how living with unresolved facial pain for so long has precipitated a serious mental health crisis, which began in October, 2019. I have been in crisis for five years.
My Mental Health Crisis

What caused my mental health crisis? Simply put, I could not endure the physical pain that I was in anymore. It was too much. The medical profession’s outright refusal to take any responsibility became unbearable. They would not listen. They would not act. This burden was too heavy to carry alone. I crashed.
I had been resilient up until October 2019. My late mother graced me with a stoic spirit that carried me through until that point. I had been going to medical appointments and articulating my symptoms to clinicians with a clear head. I did this for six years. However, in 2019, NHS trusts started to reject my GP’s referrals. They gave no reason for this. I felt invisible.
My periocular pain became particularly acute at this time. I developed throbbing pain in my temporal artery region. The pain in my remaining parotid gland was becoming more severe, and I developed ear pain on my affected side. Clinicians were refusing to see me or answer my questions. It was an impossible situation. As my facial pain intensified, so did my despair at having no medical help. After so many knockbacks, I broke. I had not experienced this level of distress before. I had known trauma from my childhood and adolescence, but I had never known this overwhelming and perpetual level of distress. A protracted crisis was new to me. My mental health crisis has lasted five years. Enduring distress for this long is exhausting.
A Vicious Circle

Mental health crisis is terrifying. The ground literally falls from beneath your feet. The word “fragility” takes on a new form. My mental health crisis has manifested in acute distress, severe insomnia, and suicidal thoughts. I have felt uncontrollable rage about how these NHS trusts have behaved, but my most predominant feelings are despair and helplessness. I explain in On Medical Trauma that I am in a constant state of shock and hypervigilance. These emotional states are also major components of my mental health crisis.
When my mental health crisis began, it did feel like everything caved in. The absence of any medical care left me feeling unsafe and frightened. This was made worse by the fact that I have had no one in the system to turn to for help or support. There has been no one to advocate for me. Doors close one after the other. As one NHS trust after another has closed my case, my mental health crisis has worsened. As clinicians have gaslighted me and continued to overlook abnormal pathology, my crisis levels have intensified and deepened. It’s a vicious circle.
Setting the Record Straight

I was not in any mental health crisis when my facial pain began in 2013. It’s important that this is understood. It is no secret that I had a challenging upbringing. My first novel, Lucia’s Poltergeist, is about the difficulties I experienced growing up. It’s not a secret that I suffered abuse at the hands of two damaged parents. However, I had dealt with my childhood issues long before my facial pain began. I had had years of psychotherapy, and I was doing well. There is no mention of suicidal ideation on my medical records before 2019. The first entries of suicidal ideation on my medical records start in October 2019.
Discrimination

I have spoken openly in this blog about the systemic mental health discrimination that I have experienced. Mental health discrimination has worsened my mental health crisis.
The lack of resolution to my facial pain and the medical gaslighting by clinicians have caused my mental health crisis. Not the other way around. I am not imagining my facial pain. However, clinicians don’t understand this. Clinicians attribute my “distress” to unwarranted “anxiety” or to “mental health” problems. They don’t join the dots. They fail to understand that my distress is being caused by not being believed by clinicians about my facial pain. The lack of self-reflection that clinicians demonstrate deepens my distress levels as I feel more unheard.
On top of the lack of empathy that I have received, clinicians have directly discriminated against me by either refusing to see me, stonewalling me for months on end, or writing inappropriate comments about me having “psychiatric problems” on radiology forms. This has exacerbated my feelings of despair.
Torture

To not be able to get answers about one’s health is a form of torture. The pain around the left side of my head now feels sinister. It feels like someone is drilling a screw into my head. Meanwhile, NHS trusts have information on their files that shows there is abnormal pathology. They have chosen to ignore this evidence, take no action, and give me no treatment. This feels inhumane.
I liken being in crisis to treading water in the Atlantic Ocean. I have nearly drowned. Waves have washed over me, and I have struggled to come up for air, but I am still straddling the waves. I am out of breath. I am exhausted. There are days when I cannot feel my own legs, but I keep going in the naïve hope that a lifeboat will see me and get me out of these perilous unforgiving waters.

The Doctor-Patient Relationship

I cannot emphasise enough how is dangerous when a clinician does not take a patient’s physical symptoms seriously. It is a form of gaslighting. It can worsen a patient’s despair. Each time that a clinician has told me that I am imagining things or that the pain I am experiencing is not real, my mental health has spiralled downward.

Relationships are a mirror. They are a two-way street. Both parties need to be honest and open with one another in order for a relationship to work. The doctor-patient relationship is no exception. However, the doctor-patient relationship toolkit, which the British Medical Association published, states that ‘the onus is principally on the health professional to make contact with patients work well.’[3] It states that ‘while doctors and patients should both be honest in their communication with each other, doctors have specific, patient-focused duties.’ [4] Doctors must:
- Treat every patient considerately.
- Listen to patients.
- Make the care of the patient their first concern.
- Give patients information in a way they can understand.
- Respect the right of patients to be fully involved in decisions about their care. [5]
None of the forty plus consultants who I have seen have listened to me, treated me considerately, given me any information, or involved me in any decisions at all about my care. The last NHS trust who refused to see me didn’t even let me or my GP know that they had rejected my GP’s referral.
Good doctor-patient relationships are characterised by mutual respect, open and honest communication, and respect for the dignity and choices of patients.
The British Medical Association.
Reflection

I have fallen into a mental health crisis because of a lack of listening and respect from the medical profession. As I say in Good Medical Practice #3, there needs to be stricter regulation to ensure that doctors follow this guidance. Medical skills and knowledge on their own are not enough. The relational workings of the dynamics between doctor and patient are just as important. It is part of patient safety that healthcare professionals adhere to the guidance about the doctor-patient relationship. A strong working relationship between doctor and patient is key to successful health outcomes.
Modern medicine is complex and dynamic. Although highly specialised, technologically sophisticated and often delivered by multi-disciplinary teams, strong doctor-patient relationships are at the heart of good care.
The British Medical Association.
Conclusion

My facial pain is a physical condition. It has a medical/biological cause that medics have not yet identified. My facial pain is not a mental health-related condition. I am in a mental health crisis because medics have not resolved my pain. This must be understood. The mental health crisis that I am in is a human response to extreme adversity. Anyone who had taken this many knocks would eventually crash. There is nothing “extreme” or “unreasonable” about feeling despair and distress at not being heard by the medical profession when I am in this much pain.
The healthcare system needs to acknowledge the impact that their decisions have had on me. Just an acknowledgement would suffice. I am a human being. I am not bionic. The human condition is fragile, and I have buckled. For my mental health crisis to subdue, a medical professional within the UK healthcare system must take responsibility for this. Until they do, I will remain in a perpetual state of crisis and, quite possibly, won’t make it. I cannot carry this burden indefinitely. I am not Superman.

Good therapeutic relationships, whether face-to-face or remote, are characterised by partnerships between doctors and patients.
The British Medical Association.
Foot Notes
[1] Psyche Hub: What is a Mental Health Crisis?
[2] Crisis Symptoms, Causes and Effects www.PsychGuides.com
[3] British Medical Association, The Doctor-Patient relationship toolkit, Chapter 2, www.bma.org.uk
[4] This quotation is from the same source as footnote 3.
[5] This information is from the same source as footnote 3.
Photo Credits: Austrian National Library and National Cancer Institute on Unsplash. Wikilmages, Granderboy and Abdou Moussaoui on Pixabay. Reneterp, David Garrison, Ayyub Jauro RDNE Project, ShotbySylvesterabigail and Cottonbro on Pexels.

2024-11-13 06:38
On Bartonella Infection
Disclaimer: This blog post is based on my experiences as a patient. I am on a long-haul journey to find answers and resolution to a chronic condition that I have suffered with for 11 years. I am not medically trained. While I have researched this subject matter carefully, this post does not provide medical advice. If you are suffering from symptoms that you think a chronic infection may be the cause of, then please consult a medical professional.
Introduction
Bartonella infection (Bartonellosis) is an infection that biting insects, such as fleas, ticks, or lice, transmit to humans. Contaminated bites and scratches, such as cat scratches can also transmit Bartonella infection. ‘Bartonella infection causes severe clinical syndromes in humans. The three pathogens responsible for the majority of Bartonella infections are B henselae, B quintana, and B bacilliformis.’ [1]
There are three subdivisions of the Bartonella infection: 1) Carrion’s disease, which Bartonella bacilliformis causes. 2) Cat scratch disease (CSD) (Bartonella henselae); and 3) Trench fever (Bartonella quintana). Culture, serology, or histopathology establish the laboratory diagnosis of Bartonella infection.

Somebody on X (formerly Twitter) has reached out to tell me that he thinks that there is a 90% chance that I have a Bartonella infection. It was the contact that I had with this person that inspired me to write this blog post. This post examines what a Bartonella infection is and discusses its causation, symptoms, and the main investigations that doctors use to identify it. It also highlights the congruence between the Bartonella henselae form of Bartonella infection (cat scratch disease) and my atypical symptoms, particularly the chronicity of my condition and the undetected aetiology. This post asks: Do I have a Bartonella infection?
Investigations.

The investigations that clinicians order to test for Bartonella infection are:
- serology: Bartonella henselae (cat-scratch disease [CSD])
- culture: B henselae (CSD)
- aspiration or biopsy of lymph nodes (CSD)
- serology: B quintana (trench fever) [2]
I have written a lot about my 11-year diagnostic delay. I speak about a common pattern over these 11 years, with medics ignoring my blood test results. This has been most common when my neutrophils and white cell count have been abnormal. My additional vexation is that medics have not carried out blood tests, which identify rare infectious diseases, like a Bartonella infection.
Doctors have ordered many blood tests to monitor my full blood count. However, they haven’t done any blood tests to look for specific infectious diseases, apart from two Lyme disease tests that I had back in 2013. They have never done a serology for Bartonella henselae. I have neither had an aspiration nor a biopsy of my lymph nodes. After my parotid surgery in 2018, clinicians missed a major opportunity. A maxillofacial surgeon removed some of my parotid tissue, in which they found dense secretions in the ducts, calcified tissue, and reactive lymph nodes (lymphadenopathy). However, they did not culture my lymph node tissue.
I have seen four infectious disease specialists over this 11-year period, who have all discharged me after one consultation. The blood tests that they ordered showed a raised white blood count and a high neutrophil count. However, clinicians did they look into these results more thoroughly. These have been missed opportunities.
Cat Scratch Disease, (CSD).

Out of the three subdivisions of Bartonella infection, I am going to focus on Cat-scratch disease (CSD) in the head and neck region because the symptoms and nature of this disease correlate most closely with the histological findings and the chronicity of my unexplained symptoms.
Cat scratch disease (CSD) is an inflammatory infection of the lymph nodes. It is a ‘benign disease characterised by regional lymphadenopathy affecting, most frequently, the head and neck region.’[3] Bartonella henselae is the causative agent of cat scratch disease. However, medics have also isolated two gram-negative bacteria, rochalimaea henselae and Afipia felis, in recent years from the lymph node tissue of patients suffering from CSD.
Cat scratch disease is an important cause of infectious lymphadenopathies in the head and neck.[4]
CSD Symptoms.

‘The most common symptoms of CSD are regional lymphadenopathy (swollen lymph nodes), fever, and malaise.’ [5] Other symptoms that fewer patients experience include encephalitis and Parinaud’s oculoglandular syndrome. Other atypical symptoms of cat-scratch disease that patients also experience in the head and neck include parotid gland swelling and swollen/infected cervicofacial glands.
Between 1997 and 1999, Ridder et al. conducted a clinical study that included 721 patients who had unclear masses in the head and neck. They diagnosed CSD by serology and molecular investigations in 99 of those patients. Cervicofacial lymphadenopathy was the most common manifestation of cat-scratch disease. They also found atypical manifestations of erythema nodosum and parotid gland swelling in 8.1% of other patients who were diagnosed with CSD.
Enlarged cervicofacial lymph nodes are a major symptom of cat-scratch disease and should be included in the differential diagnosis of lymphadenopathy in the head and neck.[6]

Woman profile facial lymphatic system nodes.
Ridder et al. also wrote a research paper on parotid involvement in cat scratch disease. Between 1997 and 1999, they observed seven patients at the ENT department in Freiburg with CSD manifestations in the parotid gland. A positive diagnosis of CSD ‘was confirmed by serology by an indirect immunofluorescence.’ [7] Ridder et al. state that ‘CSD should be considered in the differential diagnosis of all equivocal masses in the head and neck, even in unusual localisations like the parotid gland.’ [8]
Rombaux et al. argue that cervical lymphadenitis and cat scratch disease are overlooked diseases and that there is an ‘increasing incidence of patients with CSD in the ENT population and the algorithm for CSD disease affecting the cervical lymph nodes.’ [9]
Ophthalmic Complications.

There are other atypical manifestations of cat-scratch disease that involve the eyes. Ophthalmic complications of cat-scratch disease include neuroretinitis, papillitis, optic neuritis, and Parinaud Oculoglandular syndrome. Khalf, N and Lin, D explain that while conjunctival infection may last only weeks, ‘the lymphadenopathy may persist for months.’ [10]
Left periocular pain is a chronic part of my condition. I have pain and swelling all around my eft eye, which is particularly severe around my temporal artery. There is definitely no conjunctival infection now, but I do wonder if this stubborn swelling and pain could be chronic lymphadenopathy.
Calcifications.
John Ghidoni, who wrote a research paper on the role of Bartonella henselae in the nucleation of calcification, confirms that Bartonella henselae does cause calcification in soft tissue. ‘Bacterial membranes contain calcium apatite crystals. Antigenic material was present in bacteria and calcified nodules. This case illustrates calcified probiotics becoming incorporated into scar tissue.’ [11]
The soft tissue that a surgeon removed in 2018 during my parotid gland surgery had calcifications within it. Unfortunately, they did not culture the tissue to try and ascertain what bacteria had caused the hardened tissue. It was found nonetheless. I am certain that there is still calcified soft tissue on the left side of my face and around my left eye, where I experience pain. It feels rock solid to touch. I can also see in the radiology images large areas of unexplained white on the left side of my face. I have been unable to get answers about whether this is calcified tissue.
My Radiology images.

Radiology image from CT neck scan, 2020. Red arrow points to the white area on my affected side.
In my radiology images from an MRI neck scan (2022) and a CT neck scan (2020), there are areas of white on the left side of my face and around my left eye. The dense white areas that are visible on the left side of my face are not visible on my normal side. I have been trying to ascertain if these white areas are calcified tissue. If this is calcified tissue, is Bartonella henselae the cause?
Treatment.

Medical professionals recommend antibiotic treatment for Bartonella infection in order to reduce the duration of the disease, particularly in cases of severe or chronic pain. Antibiotic treatments that doctors use to treat Bartonella infection include rifampicin, ciprofloxacin, trimethoprim-sulfamethoxazole, and gentamicin.
I have tried oral rifampicin and two of the fluoroquinolones: Levaquin and Ciprofloxacin. These were effective in softening my pain. I have not tried gentamicin or trimethoprim-sulfamethoxazole. I have asked numerous times for doctors to administer intravenous (IV) gentamicin or vancomycin, but they have repeatedly said no.
Reflection.

The suspected aetiology of my illness is infection and inflammation. Bartonella henselae seems like a strong possibility as a diagnosis. Bartonella henselae is transmitted to humans by fleas and cat scratches. A fleabite to my left eye triggered my illness. Bartonella infection/cat scratch disease could account for the calcified tissue that doctors have found in my soft tissue, for my chronic lymphadenopathy, and for the involvement of my swollen parotid gland.
Left peri-ocular pain and severe pain in my parotid gland are two chronic and painful aspects of my condition. Could both my unexplained parotid gland and ophthalmic involvement could be atypical manifestations of CSD? Cat scratch disease could explain why my illness has gone undiagnosed for so long, as Bartonella hensela can go undetected for decades.
There have been clinical descriptions of cat scratch disease for over 50 years, but the bacteriologic agent was not identified for decades. [12]
Conclusion.


The persistent clinical evidence over the years relating to my condition has been raised neutrophils, WBC, and MCHC. Many research papers on Bartonella infection state that lymph node biopsy should be considered if diagnosis is unclear. I don’t understand why clinicians have never done a serology or a lab culture of my lymph node tissue. They could have cultured my lymph nodes in 2018, when the oral maxillofacial surgeon excised my parotid tissue, but they didn’t. It would be useful if medics could still perform this investigation.
Lymph node biopsy is not indicated routinely but should be considered if the diagnosis is unclear.[13]
I think the person who reached out to me on social media may be correct. I think that I may well have a Bartonella infection. Research shows that Bartonella infection causes tissue to calcify and harden. Medics have found calcified deposits in my tissue. I worry that further calcium deposits could be causing my head pain. If abnormal tissue is the cause, I am concerned that it will be too late for doctors to treat this.
I am actively seeking an infectious disease specialist who has an interest in chronic infections in the head and neck and who could look into whether Bartonella henselae is a possible cause of my facial pain. I would welcome any contact from an ID clinician from anywhere in the world.
Cat-scratch should be considered in the differential diagnosis of any acute, subacute, or chronic lymphadenopathy. [14]

Foot Notes
[1] Koirala J, MD, Sunadareshan V, MD, and Basnet S, MD: Bartonella Infection, BMJ Best Practice, June 2023, www.bmj.com
[2] This information is from the same source as footnote 1.
[3] Rombaux P et al. Cervical lymphadenitis and cat scratch disease (CSF): an overlooked disease? PubMed.
[4] Ridder G J et al. Cat-scratch disease: Otolaryngologic manifestations and management, PubMed, March, 2005.
[5] Dreher A and Grevers G: Cat-scratch disease. An overview for the ENT physician, PubMed, July 1996.
[6] Ridder G J et al. Cat-scratch disease: Otolaryngologic manifestations and management, PubMed, March 2005.
[7] Ridder G J et al. Parotid involvement in cat scratch disease: a differential diagnosis with increased significance, National Library of Medicine (NIH), August 2000.
[8] This quotation is from the same source as footnote 7.
[9] Rombaux P et al. Cervical lymphadenitis and cat scratch disease (CSD): an overlooked disease? 2005.
[10] Khalf N and Lin D: Diagnosis and interpretation of testing for cat scratch disease, Copyright © 2021 Baylor University Medical Centre, Taylor and Francis Group.
[11] Ghidoni, J.: Role of Bartonella henselae endocarditis in the nucleation of aortic valvular calcification, February 2004, National Library of Medicine (NIH).
[12] Baranowski K and Huang B: Cat Scratch Disease, StatPearls; January 2024.
[13] Khalfe N and Lin D: Diagnosis and interpretation of testing for cat scratch disease, Copyright © 2021 Baylor University Medical Centre.
[14] Ridder G J et al. Cat scratch disease: Otolaryngologic manifestations and management, March, 2005, National Library of Medicine (NIH).
Useful Videos
Photo Credits: Edward Jenner, Peyma Farmani, CDC, National cancer Institute and 42 North on unsplash. Shvets Production on Pexels. Anja from Pixabay.

2024-09-23 06:01
On Invisible Illness
Introduction
An invisible illness is a physical or mental illness that others can’t see. These illnesses include a range of energy-limiting conditions that are not visible to the onlooker. Examples of invisible illnesses include fibromyalgia, endometriosis, Chron’s disease, chronic pain, irritable bowel syndrome, myalgic encephalomyelitis (ME), diabetes, lupus, epilepsy, asthma, and arthritis.

There are also many invisible illnesses that are associated with mental health, including depression and anxiety. This post, however, focusses on invisible illnesses that have a biological or physical cause. This post explores the relationship between invisible illness and stigma. It also discusses the direct relationship between invisible illness and the difficulties we face as patients with doctors not believing us about our symptoms. It debates the day-to-day difficulties of living with an invisible illness and the importance of radical self-care.
My invisible illness

My facial pain is an invisible illness. You would not know by looking at me that I a.) have a chronic condition or b.) am in severe pain. It is not noticeable to a stranger that my pain is taking a huge toll on my mental health and stealing my quality of life. It isn’t visible or obvious that I am suffering. The disease that I have exists within the soft tissue and muscle of my face, not on my skin, so I ‘look fine.’ But I am not fine. I live with unrelenting pain.
My experience of living with an invisible illness is tough. I experience a lack of empathy, understanding, and sympathy from others. I also feel an expectation that I should “just get on with it.” This can feel incredibly lonely. I have been in situations where friends have said, ‘You don’t look like you’re in pain, or even worse, they have told me to ‘stop mithering.’ Because of my experience, I rarely speak about the pain I am in. I feel that if I talk about my facial pain, others will dismiss me. So, I keep quiet. This too, can feel lonely.
One of the most difficult and hurtful consequences of having an invisible illness is the lack of understanding from others.[1]
Radical Self-Care
 The hardest part of having an invisible illness is the lack of empathy we get from people in our day-to-day lives. The “just get on with it” mentality feels very unkind. We therefore need to have lots of self-compassion. Our disease may be invisible, but it is real. A part of our body is not functioning as it should. It is likely that our immune systems are fighting hard all of the time, making us tired.
The hardest part of having an invisible illness is the lack of empathy we get from people in our day-to-day lives. The “just get on with it” mentality feels very unkind. We therefore need to have lots of self-compassion. Our disease may be invisible, but it is real. A part of our body is not functioning as it should. It is likely that our immune systems are fighting hard all of the time, making us tired.
In my case, infection and inflammation are the suspected causes of my facial pain, and doctors have found that my parotid gland isn’t working properly. One doctor told me that he thought a pervasive infection had damaged the lymphatic drainage system in my facial region. There is a reason that I feel unwell and weak, despite my disease not being visible to others. Other people may have an ill-functioning digestive system, kidney function, or inflamed joints. The list is endless. Whatever illness we have, some part of our body isn’t working as it should.
An Analogy

Think of football. A standard football has 32 panels: 20 hexagons and 12 pentagons. If something or someone damages one of those panels, it affects the ball’s performance. The football loses its spherical shape, which leads to an uneven bounce. The football isn’t as durable as it should be. A compromised panel can also lead to further damage, causing the ball to deflate or burst during life.
Humans aren’t dissimilar to footballs. If a part of our body does not function properly, we do not have as much bounce or speed as others who have fully functioning bodies. While others may not acknowledge this, it is imperative that we do. No matter how hard you kick a damaged ball, it still won’t bounce like it should. It’s damaged. The same is true with humans. If we push ourselves too hard, we will not go any faster. We will make ourselves more unwell in the process.
We therefore need to exercise radical self-care. It is challenging to not be able to keep up with everyone else. I find it really difficult. However, to prevent making ourselves more unwell, we have to acknowledge our limitations. This takes a large dose of self-compassion. We have to be kind to ourselves. I spoke about this in On Chronic Illness and Identity. Finding self-compassion is hard, but it is a vital part of our journey. Our bodies do not work as they should. We therefore, must not push our bodies too hard. We must exercise radical self-care.
Mental Health & Relationships

There is a direct link between physical pain and mental health. Anyone who endures endless days of physical pain will have bouts or long periods of low mood. It’s miserable being in pain all the time. This can be the hardest part, I find, of self-care. We need to be tender towards ourselves when we are struggling. Maintaining relationships with an invisible illness is also not easy. If friends knew our former selves as fun and energetic, then they may find it difficult to accept the change in our disposition. Sadly, this is where relationships can fracture. The friends who have stayed with me are those with whom I can communicate openly. They also have experienced illness themselves.
Intimate relationships (romantic/sexual) can also be problematic when we have an invisible illness. The same lack of patience and understanding that one finds in friendships can also exist within intimate relationships. I have not managed to hold down a romantic relationship since my facial pain began. All I can say on this subject is that if you have a lover or partner who is supportive, patient, and accepting of your invisible illness, then wrap them up in shiny paper and keep them safe in a treasure chest. Don’t let them go!

Medical Gaslighting

I have written two blog posts about the medical gaslighting that I have experienced from medical consultants. Clinicians have told me that what I am seeing or experiencing is a figment of my imagination. These experiences have been traumatic. I have chosen not to attend any more consultations. The gaslighting is too distressing. However, I want to touch on medical gaslighting within the framework of invisible illness.
As a patient who has an invisible illness, I am certain that this has contributed to the gaslighting that I have experienced. I am able to explain to doctors what my symptoms are. I am also able to communicate how my pain affects me. However, if I look fine, then I question whether this has contributed to the dismissive attitudes that I have come up against from doctors. I also question whether my invisible illness has contributed to my diagnostic delay. Medics feel no urgency to help me because ‘I look fine.’
Open and Honest Communication

I recently listened to a wonderful interview with Anneke Vliegen, the author of the memoir Recognise ME, on the podcast ‘Post-Exertional Mayonnaise.’ Anneke spent twenty years seeking the correct diagnosis for her condition. Medics misdiagnosed Anneke with myalgic encephalitis (ME). Doctors finally gave her the correct diagnosis of Ehlers-Danlos syndrome. Anneke speaks about the medical gaslighting that she experienced over the years. She also explains that once she received the correct diagnosis, clinicians were more respectful towards her.
Anneke highlights that patients with an invisible illness are more susceptible to experiencing medical gaslighting. This is even more likely if our condition is undiagnosed. Anneke says that as patients, we need to take some responsibility and try to be as open and honest with doctors about how our illness affects us. She acknowledges that this may involve making ourselves vulnerable to clinicians. If we can be open and honest with doctors about how our illness affects us, they may understand better. She rightly explains that doctors see us for twenty minutes, and they just don’t see what our lives are like. Anneke used a functioning scale, and she would tell doctors how many hours a day she was able to function for.
Reflection

I found this insight useful. However, I have found the clinical experience threatening. This has made it challenging to be open or vulnerable with consultants. As soon as I see the stern frown and closed look on a clinician’s face, I shut down and feel unable to speak. It’s difficult to be open and honest with people when there is no vessel open for authentic communication. Anneke’s theory is certainly something to aspire to. I do, however, think that both doctor and patient are responsible for open and honest dialogue. Not just the patient.
Stigmatisation

For those of us who have an invisible illness, especially with no diagnosis, we do come up against stigma within the medical community. In The Wilderness of Medically Invisible Disability, Catherine Hale from the Chronic Illness Inclusion Project talks about an article in The British Medical Journal that a GP and trainee psychiatrist called Lisa Steen wrote. Lisa Steen developed symptoms of a rare cancer that went undetected for a long time. Standard diagnostic tests could not explain her symptoms. Doctors diagnosed her symptoms as health anxiety. By the time they finally diagnosed her cancer, it was too late for them to treat it, and Lisa died shortly after writing her article, which she called Wilderness of the medically unexplained.
Lisa’s article is about patients who have physical symptoms that, like me, she was sure had an organic cause, but that health professionals doubted and dismissed. Lisa describes conversations with fellow doctors as feeling like “a goldfish with no voice.” She writes of watching doctors’ faces glaze over at her multitude of symptoms. I know that glazed look!
Catherine Hale speaks about Lisa Steen’s case. ‘Lisa acquired a stigma because medical professionals labelled her symptoms as medically unexplained,’ Catherine says. ‘The way that stigma works is that you believe that there’s something about your disease that makes you less credible as a person, and that makes you feel ashamed. There’s nothing shameful about us or our disease. Stigma is a form of oppression that unequal relationships impose on us. The inequality is about who has the authority to know things about our bodies. That authority admits no possibility of failure. So, when lab tests cannot detect our illness, a kind of flawed logic kicks in that says our disease doesn’t exist.’[2]
Reflection

Catherine’s words resonate with my experience over the last 11 years, consulting with clinicians. There is an inherent link between stigma and invisible illness. I have definitely faced stigma from doctors. Having an invisible illness definitely contributes to doctors not believing us about our symptoms. It also contributes to the delays that we experience in acquiring a correct diagnosis. For those of us who suffer with invisible illnesses, stigma is very real. I think that stigma has played a critical role in my negative experiences with medical professionals.
Conclusion

The challenges of living with an invisible illness are very real. The lack of support and empathy from others, coupled with the stigmatisation from doctors, makes it a lonely experience. Self-compassion and self-care are qualities that we must strive to foster. Our medical conditions are real, even though they may not be visible to others. Only we know how our conditions impact our lives, so kindness towards oneself is key to our survival and livelihood. Being kind to others, who suffer with an invisible illness is imperative too! Learning to be our own advocate is also essential. As difficult as this can be, these are our bodies. These are our lives, so we must keep speaking until we find the right doctor who can accompany us on our journey to better health.
Constantly feeling as though we need to prove that we have challenges can be frustrating and exhausting, especially when we’re running on empty. We frequently deal with a multitude of questions about our illness and this can be draining. These questions cause us to doubt ourselves. When others assume it’s all in your head, it can make you question your reality. [3]

Foot Notes
[1] Collins-Burke A, RN; The Challenges of Living with an Invisible Illness, April, 2021, Psychology Today.
[2] Hale C and Allam A; The Wilderness of Medically Invisible Disability, The Chronic Illness Inclusion Project, 24 May, 2022. This talk was part of the Disbelief and Disregard webinar at Liverpool University.
[3] This quotation is taken from the same source as footnote 1.
Recommended Videos
Photo Credits; Avi Agarwal on Unsplash. Pexels, unknown, Tumisu, Open Clipart-Vectoria, Self detective on Pixabay. Gui Spinardi, Fotios Photos, Katie Rainbow, Eric W, The fullonmonet, Mart Production and Cedric Fauntleroy on Pexels.

2024-09-09 09:42
On The Falsifying of My Medical Records #3
This blog post contains wording about suicide that some people may find triggering. If you are in the UK and need urgent help, please call 999. If you need support, please call 111 (option 2) or Samaritans freephone: 116123.
Introduction
In On the Falsifying of My Medical Records #1 that I published on 29 June, 2024, I recounted five serious incidents where my GP Practice has falsified my medical records. The incidents involve the GP practice amending a record 18 months after it was made, deleting a record, falsifying two records, omitting a record, and deleting and then re-entering a record. I explain in On the Falsifying of My Medical Records #2 that these incidents breach GMC guidance and The Data Protection Act, 2018.

I am writing this post with a further two incidents that have occurred since 29 June 2024. In this post, I recount these incidents with supporting evidence, where my GP practice has falsified my medical records and breached GMC guidance once again. While one of these incidents is not directly linked to my facial and periocular pain story, it is linked to the narratives of my medical story. These narratives are NHS bodies neglecting their duty of care, appearing to cover for one another, and lacking transparency.
Incident 6: Context

Photo of rash that I developed on my right hand in June, 2024.
On 26 June 2024, I developed a rash on my right arm and hand. I sent an email to my GP practice, in which I asked them to prescribe something for the rash and I included 15 clear photographs of the rash.
I didn’t hear anything back from them, so I emailed them on 3 July (one week later) asking them for an update. The GP practice emailed to say that they aimed to ‘get the issue resolved as soon as possible.’ They told me that they had sent the photos to a “clinical pharmacist.” They said that they were waiting for his opinion.
On 18 July, I still had not heard back from them with an update or a prescription. My rash was worsening. I contacted the GP practice again and told them that the rash was itchy. I requested some cream or medication, and I received an email from one of the doctors at the practice.
The Email Said:
Dear Felicia,
Thanks so much for your message.
I’ve just seen the photos of your skin rash that you sent in 3 weeks ago. I think the clinical pharmacist was going to get back to you, but I’ve just had a look at the pictures after I was sent a task by our secretaries today.
The rash does look sore. I wonder if the rash higher up your forearm might possibly be urticaria, which can sometimes be triggered by an allergy. The rash on your hand looks slightly different.
I’ve prescribed you some more Fexofenadine tablets for the itch, and I would advise trying Eurax 10% cream on the rashes, which can be soothing/settling for such rashes. I’ve sent the prescription for this to the pharmacy now.
I’ll also ask Dr. for her opinion, as she has a special interest in skin conditions.
Best wishes,
Dr
Falsifying A Record

The Eurax cream had no effect, and my rash continued to worsen. I did not hear anything from the clinical pharmacist, and the GP did not get back to me, regarding consulting with his colleague, ‘who has a special interest in skin conditions.’ I booked an appointment to see a dermatologist at a private hospital.
On 9th August, I saw the dermatologist privately. She diagnosed my rash as dry eczema, and she gave me a ‘Treatment Request Form’ to give to my GP to prescribe a 100-mg tube of Elocon ointment (Mometasone Furoate). The appointment with the dermatologist cost £200.00.

GP Treatment Request Form that the dermatologist told me to give to my GP
On 12 August, I sent an email to the GP practice with the ‘Treatment Request Form’ that the dermatologist told me to give to them. The GP practice sent me an email saying that they would prescribe the cream that my dermatologist requested. They did dispense the cream that day.
When I logged into my System One online portal, I saw, again to my horror, that the clinical pharmacist, who I never heard from, had entered onto my record that he had prescribed the cream and that he had seen me. The record said:
12 August 2024; seen by clinical pharmacist, (Y20a6)
The clinical pharmacist hadn’t seen me. I have never seen or spoken to him. I do not know who he is. This is a false record.

A screen shot of my medical records, showing that the pharmacist falsely recorded that he saw me. I don’t know who he is. He didn’t see me.
Falsification is often an attempt at damage control for a known error or an adverse outcome. [1]
Incident 7:
Omitting Significant Facts

I have been suffering with suicidal ideation since 2019 because of the intensity of my undiagnosed facial pain and because of the constant obstacles that I have faced from the healthcare system in accessing treatment for my facial pain. My suicidal ideation has intensified in the last few months, but my mental health team has discharged me, so I have no support. I have been to A&E on a number of occasions to get help for my suicidal thoughts. I recounted in my first post on the falsifying of my medical records how my GP practice deleted a record that documented that I went to A&E on 17 May 2024 because of my ongoing suicidal thoughts.
On August 27, 2024, I went to A&E about my suicidal thoughts again. I saw a mental health liaison officer who assessed me and said that she was going to write to the Community Mental Health Team (CMHT) and ask them to see me again and that she was going to write to my GP and ask them to review my sleep medication because I am sleeping, on average, 1 hour a night. This is because of severe head pain, which is keeping me awake.
The Omitted Fact

On my medical record, my GP practice has omitted a significant fact regarding my attendance at A&E on 27 August. The GP practice has recorded that I went to A&E for an ‘ongoing episode.’ However, they have not stated what I went to A&E for or what that ‘ongoing episode is.’ They haven’t said that I went to A&E for suicidal thoughts.
The records state:
27 August: Seen in accident and emergency department (9N19) (Ongoing Episode.)

My medical record; the GP recorded that I was seen in A&E for an ‘ongoing episode,’ but they have omitted the reason why I was seen and have not said what the ongoing episode is.
The summary from my attendance at A&E on 27 August, which shows that I attended for ongoing suicidal feelings. Not stated by GP on record above.
Falsification and tampering come in many forms—removing a diagnostic report, inserting information without standard documentation, rewriting or destroying the record, and omitting significant facts. [2]

Serious Concern

I am disturbed that my GP has omitted something as serious as my suicide risk. The GP practice has falsified my medical records in varying degrees seven times now. To experience this abuse of power first-hand as a patient is alarming and distressing. I am concerned that my records are missing vital information.
My immediate concern is how much other data the GP practice has potentially destroyed. Each time that I have attended A&E for suicidal feelings, a mental health liaison officer has written to the GP. I am concerned that my GP practice has either destroyed or not uploaded some of these letters to my medical records. I am most concerned about the letter that the liaison officer sent to my GP on 17th May 2024. It was this visit to A&E on 17th May that the GP deleted from my medical record. (They have since added an administration note to my record after I spoke out about this incident on social media on 3rd July.)
Good Medical Practice

Good medical practice states that a doctor ‘must’:
51 You must put patient safety first at all times.
Record Keeping
69 You must make sure that formal records of your work (including patients’ records) are clear, accurate, contemporaneous and legible.
70 You should take a proportionate approach to the level of detail, but patients’ records should usually include:
a relevant clinical findings
b drugs, investigations, or treatments proposed, provided, or prescribed
c the information shared with patients
d concerns or preferences expressed by the patient that might be relevant to their ongoing care, and whether these were addressed
f decisions made, actions agreed (including decisions to take no action), and when/whether decisions should be reviewed
71 You must keep records that contain personal information about patients, colleagues, or others securely and in line with any data protection law requirements.
Patient Safety
73 To help keep patients safe you must:
b contribute to adverse event recognition
c report adverse incidents involving medical devices (including software, diagnostic tests, and digital tools) that put the safety of a patient or another person at risk or have the potential to do so.
d contribute to incident reviews and/or investigations. [3]
Breaching Guidelines

These recent incidents are a breach of Good medical practice. GMC guidance states that doctors must ensure records are accurate. It is not accurate that the clinical pharmacist ‘saw me’ on 12 August. I’ve never met the man, and omitting the reason I went to A&E is neither accurate. The GP practice should have clearly stated the reason that I went to A&E and stated what the ‘ongoing episode’ is on my records. A new medical professional looking at my record would have no idea from that entry why I went to A&E or that I am suffering with suicidal ideation.
GMC guidance states that you must put patient safety first at all times and report adverse incidents that have the potential to put the patient at risk. Omitting such a serious fact from my records is not putting my safety first. It does the opposite. It puts me, the patient, at higher risk. Attending A&E for suicidal thoughts is an adverse incident. The GP should have accurately reported this on my medical records.
Conclusion

It is difficult to find the words to express how it feels to be at the receiving end of conduct like this. It is saddening that the GP practice has omitted such serious information from my medical records. I am hurt that they are acting as if I do not exist. I do exist. However, they are ignoring and downplaying my reality. I feel invisible, which is contributing to and worsening my suicidal feelings.
Change and reform must come. I would like to see a system that prohibits conduct like this and in which a GP would not dare consider doing what my GP practice has done. The change must bridge the gap between words on paper and reality on the ground. Real change would mean that the term “patient safety” would not just be a platitude, a politically correct term that is spouted by politicians; it would be a reality that is enforced by far greater surveillance and stricter regulation.
Doctored data can throw into doubt the basis of a diagnosis, the treatment plan, and communications with patients, which can have serious implications for the quality of patient care. [4]

Blog Post Update.
Today is 14 November 2024. I published this blog post on September 9, 2024, just over two months ago. Since publishing this post, my GP practice has tampered with my records again. They have amended one of the entries to my medical records without being transparent about why they did it.
I explain in incident 7 that after I attended A&E for help with suicidal thoughts on 27 August, my GP practice omitted vital data when they recorded my visit to A&E. The GP practice recorded that I went to A&E for an ‘ongoing episode’, but they did not state what that ‘ongoing episode was.’ They did not state that suicidal ideation was the ongoing episode. On August 27, the record that they made said: Seen in Accident and Emergency (9N19) (ongoing episode). That was it.

This is how my record looked on August 27. It said ‘seen in Accident and Emergency’ ‘ongoing episode.’ You can see from the edges of the photo, that that was the end of the record. They added nothing more. I have not cropped the top of it.
I published this post (September 9). When I logged into my System One account last week, I saw that the practice had amended the record. The GP practice added to my record that suicidal ideation was the ‘ongoing episode.’ First, this indicates that my GP practice is definitely reading my blog. Secondly, they have been dishonest. They have dated the new record to 27 August. However, they did not make this amendment on 27 August. They made it between September 9 and today. The GP practice did not indicate who made this amendment and why they did it. This is expected of all medical professionals. The record looks like this today, 14 November 2024.

The red arrow shows where the GP practice has added what the ongoing episode was. The practice did not make this record on 27 August, as it says they did. They did this after September 9.
This is the eighth time that my GP has falsified my medical records.
Foot Notes
[1] Falsifying Medical Records | Med Law Advisory Partners Med Law Advisory Partners
[2] Medlaw Advisory Partners: Falsifying Medical Records, February 2021, About Us | Med Law Advisory Partners Med Law Advisory Partners
[3] General Medical Council: Good Medical Practice, January, 2024. All of the citations in this paragraph are taken from this source.
[4] Thompson Jayne, LL.M: What Are the Consequences of Falsifying Medical Records? December, 2018, www.legalbeagle.com
Photo Credits: StockSnap, Fathromi Ramdlon, Gerd Altman and Alexandra Hal on Pixabay. CottonBro studio, Tima Miroschnichenko, Mikhail Nilov, Anete Lusina and Chuck on Pexels.

2024-08-29 08:49
Professor Swinford
Professor Swinford is an excerpt from my medical memoir – a work in progress. The genre is creative nonfiction. It is based on real-life events. All names have been changed to protect the identity of the individuals involved. Professor Swinford is a fictional name in place of the professor who I saw.
Chapter Five
London
July, 2014
Professor Swinford was the professor of ophthalmology, to whom Mr Badawi referred me. I had to move to a new GP practice first so that I could get the second referral that Mr Badawi explained that I would need. I contacted NHS England, and explained my situation to them. NHS England registered me at a new GP surgery. The new surgery accepted me as a patient under the agreement that I did not request home visits because I was out of their catchment area. A locum GP at the new GP practice seconded Mr Badawi’s referral to Professor Swinford. My first appointment with him was in July 2014 at a large NHS teaching hospital in London.

I had a horrid taste of metal in my mouth as I waited for Professor Swinford to come and get me from the waiting room. He was small, with short, curly grey hair and a distinctive pimple on his cheek. Underneath his stained white coat, he wore casual attire, jeans, and a checked shirt. He looked like he was in his early sixties and walked with a limp, which I noticed as I followed him along the lengthy corridor to his consulting area.
The ophthalmology clinic was a large open-plan room with no windows. There were ten ophthalmic consulting stations dotted around the sides of the room, where ophthalmologists with different specialities saw patients. At each station, there was a black leather examination chair, a slit lamp, a phoropter, a retinal camera, and an ophthalmoscope. There was a close smell of acidic substances and a more distant stench of mashed potatoes.
The Consultation

The clinic was busy. I could hear conversations between clinicians and patients that were taking place around us. We sat face-to-face under a bright spotlight. I sensed a barrier from professor Swinford, which I suspected came from him reading the notes that Mr Badawi sent him. He knew it was a ‘complex’ case. Professor Swinford was a well-spoken man. He talked in a quiet tone, but he maintained eye contact with me when he spoke. I told him about the pain that I was feeling around my left eye, particularly around my temple area.
‘What are you currently taking for pain control?’ he asked.
‘Rifampicin,’ I replied. ‘I feel better than I did, but it’s not getting rid of the pain around my eye.’
His eyes scanned my left eye region. ‘Let’s take a closer look at your eye,’ he said. I rested my chin on the ophthalmoscope. He twisted the dial so that the bright light came right up to my retina, making it challenging not to blink. ‘Everything looks OK inside your eye,’ he said.
My Left Ptosis

This photograph shows my left ptosis, (my smaller left eye where the levitator has collapsed.)
I asked Professor Swinford about my small left eye. ‘It hurts,’ I said. ‘It’s smaller than my right eye.’
‘Yes, you’ve got a left ptosis,’ he said.
‘What’s a ptosis?’ I asked.
‘The levitator muscle on your eyelid has collapsed.’
The memory of when my eyelid collapsed was still close. It was shortly after I had finished using the Maxitrol eyedrops, and I had that awful sensation of worms wriggling in my lower eyelid. I was standing in a sunny hotel room in Southport, and my left eyelid fell.
‘Can you do anything about it?’ I asked.
‘It needs corrective surgery.’ Using his middle finger and thumb, he raised my upper eyelid to where it should be.
‘That feels better when you do that,’ I said.
‘Yes, it will feel better, but it’s not safe for you to undergo corrective surgery while you have these symptoms. It could make matters much worse for you.’
‘Is there a surgeon at this hospital who could do it?’ I asked.
‘Yes, we have an excellent oculoplastic team here who could correct it.’
Professor Wong didn’t tell me about my ptosis. I felt a wave of nausea thinking about that intimidating meeting with him and his colleagues in January 2014. I had shown him the photo on my BlackBerry phone of my small eye, but he shooed me away, like I was a stray cat. It was a relief that Professor Swinford had diagnosed my ptosis, but I was frustrated that he had no interest in finding out what had caused my levitator to collapse. I wanted to find out what was causing the pain and swelling around my eye and cheek, and my symptoms in general.
Resistance

I could feel the resistance from Professor Swinford to diagnose and treat my condition.
‘What about the swelling around my eye?’ I asked. ‘It hurts.’
‘Yes, I can see the swelling. It’s the soft tissue, that’s the problem.’
‘Can you help with that? I’m in a lot of pain.’
He shook his head tersely. ‘I don’t deal with soft tissue problems. I specialise in uveitis, which is inflammation of the eye itself. You don’t have that. Your problem is with the tissue surrounding your eye.’
What I found hard to fathom was the lack of curiosity, a wider intelligence, a desire to help, or a general feeling of care that these medics didn’t have. They were nonchalant. They found a way out of having to take any responsibility for my clinical problem. I had severe pain and swelling around my eye. Professor Swinford was a professor of ophthalmology with a notable reputation who had identified that I had a problem with the soft tissue and that something had caused my levitator to collapse. He had a team of 20 clinicians under him who could have helped me, but he used a feeble excuse for not helping, saying that this wasn’t “his speciality.”
Surprise

He did surprise me, though, with an outburst of anger mid-consultation about the fact that they weren’t treating me up north.
‘Why are you down here seeing clinical teams? Why aren’t they treating you back up north?’ He asked with reddened cheeks and a stern frown.
I started to speak, but I tripped on my words.
‘Why are you paying all of this money to see this private rheumatologist? Why are you paying for your antibiotics?’
I looked at him head-on, ‘Take that up with your colleague, Professor Wong,’ I said. ‘He will fill you in.’
No more was said.
‘Keep taking the Rifampicin,’ he said. ‘What about steroids. Have you tried them?’
‘Yes, I have tried oral Prednisolone, but it made things worse.’ I replied.
‘Would you be willing to prescribe linezolid. It really helped me before,’ I said.
‘No, he said, shaking his head. I won’t. I’ll keep you monitored and see you again in 3 months’ time. We’ll see how things are then.’
It was busy on the Embankment when I exited the hospital. There were mime artists entertaining groups of tourists and buskers playing music. My first appointment with Professor Swinford left me with mixed emotions. I was relieved that one piece of the puzzle had been found (my ptosis), but angry that he wasn’t going to address the actual problem. He told me the truth, in part, but he also chose to turn a blind eye to a clinical problem that he identified.
Reflection

I noticed when I saw Dr Bhan again, who had received a copy of Professor Swinford’s clinic letter, that he was more attentive now that there was a diagnosis of my ptosis and that Professor Swinford said to continue taking the rifampicin. Clinicians work together under a system of agreement and do not like to wrong-foot one another. They follow one another’s opinion, even if it is contrary to what the patient is saying.
I was up and down from Yorkshire to London a lot over the summer months of 2014, and I needed to find somewhere to stay when I came for my appointments, which were in south-east London. I found somewhere that became very dear to my heart, and I began a new and long-lasting love affair with the city in which I am from.

My Mother’s Legacy

My mother was frugal. She was a posh bird by trade, but she was none the comfier, tucking into a chicken salad and drinking a mug of ‘builder’s tea’ at the local community café. If I tried to egg her on to go to the Hungarian café on Finchley Road, she wouldn’t have any of it. She was from a well-to-do Jewish family, but she had a no-frills approach to life. Two failed marriages had left her bereft of wealth. She was a single mother of three children, whom she raised on a part-time wage as an NHS receptionist, so she had to watch the pennies.

My mother was a thrifty woman. She would banter with the fruit and vegetable stallholders at Swiss Cottage Market and could always get a few pennies knocked off a pound of tangerines. Growing up in the Primrose Hill area, most of my friends came from wealthy families. I couldn’t afford the latest Nike Air Max trainers as they all could, but my mum’s thriftiness made sure that I could just about keep up to speed with the latest trend. We would go to Queens Crescent Market early on Saturday mornings, where she would find me a pair of knock-off Nike trainers that looked like the real deal for under a tenner. Because of my upbringing, I gravitate generally towards ungentrified places, where bankers have not yet turned old muck into shiny gold.
Walworth Road

East Street Market, a street market in Walworth in South East London
I found my slice of heaven in the Walworth Road area of Elephant & Castle. Walworth Road was lined with greasy spoon cafés, electrical discount shops, pawn brokers, and, of course, East Street Market, where you could get a bag of apples and pears for under a fiver! Not a Costa Coffee in sight, I felt at home here, even with the sound of sirens constantly whizzing by.
I found a hostel in that area. It was in an old converted church with airy rooms that had steeple-like ceilings. Depending on the time of year, it could be quiet with one or two travellers, or it could be heaving with big groups of tourists. The manager knew that I was coming down to London for medical appointments, and in the winter months, when the hostel was quiet, he would give me a wink; room 12 is empty. It’s all yours, darling.
Then I got a dormitory all to myself. Mostly, I was in crowded rooms with overweight men who snored, but this was my home when I came to see Dr Bhan or Professor Swinford. I travelled by Megabus from Bradford to London the day before my appointment, headed to my hostel, got a box of curried goat and rice from the Jerk Chicken shop, and bedded down for the night.
I fell in love with southeast London. It wasn’t a part of London that I had explored before. Camden and Islington had been my stomping grounds during my teenage years, and where I had spent most of my time, while growing up. It was great to discover areas like Tooting, Greenwich, and Deptford, all understated places buzzing with diversity, and there were no memories of my past in this part of London. It was a blank canvas to explore.

A Pattern of Behaviour

I could see a pattern of behaviour emerging with these medical professionals. There was evidence that there was a clinical problem. They knew that there was something wrong, but doctors don’t like cases where patients have seen a lot of other professionals. My case was not attractive. I don’t think that they had anything against me, but there was an invisible wall that was erecting before me, a wall that was built on a silent agreement between these clinicians to not name or diagnose what was wrong, because to diagnose or name it would be to admit fault somewhere along the line. It was playing out like a game of Chinese whispers.

There was a definite defensiveness coming from medical consultants, but with my body reminding me every second of every day that there was something wrong, I had a duty to push against their collective resistance.

Recommended Articles
Episode 15: Memoir as a Political Act – The Nasiona
The Aesthetic Memoir: Interview with Lorelei Golding – Lily Dunn
The Aesthetic Memoir: Interview with Susanna Crossman – Lily Dunn
Photo Credits; Tima Miroshnichenko, Olgalioncat and Suzy Hazelwood on Pexels. Sander Sammy, Jon Tyson, Dylan Nolte and Christina Langford Miller on Unsplash. Leroy Skalstad, Roszie, Andrew Martin and Norwich-blueprint on Pixabay.

2024-08-28 06:31
Dr Bhan
Dr Bhan is an excerpt from my medical memoir. This is a work in progress. The genre is creative nonfiction. It is based on real-life events. All names have been changed to protect the identity of the individuals involved. Dr Bhan is a fictional name, in place of the doctor who I saw about this issue.
Chapter 4
London
May, 2014
It was a long train ride down to London to see Dr Bhan. I was weak. Walking was an effort. The left side of my face was so sore that I was unable to sleep on my left side. My jaw region was rock hard, and I had chills rushing up and down the left side of my face. I felt nauseous and downright awful.
The night before my first appointment with Dr Bhan, I stayed in a hostel in Kennington, not too far from London Bridge. It was on a leafy street. There was a café next door. It resembled cafes that I had been to in San Francisco. There was ambient dub music playing, and there was a solo cyclist sitting, drinking coffee while web browsing. I was sharing the dormitory that night with two Japanese women, and I was in and out of the toilet, throwing up most of the night.
‘You sick?’ one of the women asked.
‘I’ll be OK,’ I replied. ‘I’m seeing a doctor tomorrow.’

A Private Hospital
The private hospital was within walking distance of London Bridge station. It was a tall building with large stone pillars in front. This new team were rheumatologists. Their speciality was connective tissue diseases, mainly Lupus and Sjogren’s syndrome. I wasn’t sure why Mr. Badawi had referred me here when I had a suspected soft tissue infection. But I walked through the door anyway, in the hope of some help.

The doorman was a beautiful-looking Ghanaian man named Dodzi, who flashed me a welcoming smile as he opened the door for me. The building smelt like grapefruit mist, and it had an old-style birdcage elevator with a manual scissor gate. I exited the lift on the second floor to a waiting room with plush brown carpets and large windows that overlooked the River Thames. The concierge was a short, middle-aged guy. He was called Graham. He booked me in for my appointment. Graham had a broad Bermondsey accent, which made me feel immediately welcome.

The back of my neck and the palms of my hands were sweaty as I waited nervously for Dr Bhan to call me. Dr Bhan was a rheumatologist. He was a tall man of Indian descent who was wearing a pair of casual chinos and a burgundy tank top. He appeared at the door of the waiting room with a wide-open smile and sparkling white teeth. ‘Felisha Solomon,’ he called, and he led me along a corridor to his beautiful consulting room. I had never seen a doctor’s room like this before. It was huge. There were large windows behind his desk, out of which there was a cinematic view of Tower Bridge and beyond. The sky was belting blue, and this expansive vista inspired a feeling of hope in me.
The Consultation

‘Please take a seat,’ he said politely.
There was a stream of my medical records on Dr Bhan’s desk. Mr. Badawi had faxed them across. Dr Bhan clearly knew the backstory with Professor Wong. However, with a consultation fee of £195.00, I hoped that he would give me a decent hearing.
‘I’ve had a read-through of the story so far,’ he said. ‘Where exactly is your pain now?’
‘It hurts around my eye and jaw area,’ I replied, ‘my jaw feels rock hard and it hurts to open my mouth.’ I told him how ill I felt and about the chills running up and down the left side of my face. I also explained that I had not had any medication for five months since Professor Wong stopped my treatment.
‘You do look ashen-white and very unwell,’ he said. ‘I want to do an examination of you and do some urgent blood tests to see what’s going on.’
Dr Bhan was well-spoken. He had a deep and soothing voice, and he emanated a charm and professionalism that you couldn’t fake. I didn’t know where in India Dr Bhan was from. I thought that he perhaps came from the Kashmiri or Punjabi region. His face was narrow, and he was light-skinned. He didn’t have the darker shade of skin of the Tamil people. I lay on an examination table. Dr Bhan prodded my abdomen and groin area. He examined all of my joints but he then spent most of the time examining the area around my left jaw.
‘Your masseter area does feel very tender, he said. ‘I can feel that there’s something there.’
Blood Tests

I got dressed. Dr Bhan returned to his desk to jot down some notes. ‘Can you tell me which antibiotics you have tried?’ he asked.
‘I have tried most of the macrolides and doxycycline.’
‘Let’s get some blood tests done, and then we’ll come up with a plan,’ he said, handing me a green slip. ‘I’ve requested a full blood count, along with your ESR and a renal and liver function test. I also want to see what’s going on with your antibodies and electrolytes. Once they have done your blood tests, just return to the waiting room. I’ll come and get you.’ His politeness was such a welcome contrast to the volatile disposition of Professor Wong.
I made my way along a carpeted corridor to the blood test room, where a smiling phlebotomist was waiting for me. Rafael was from the Philippines. He had been in England since the age of 14. He had an infectious smile and a magical way of distracting my attention away from the prick of the needle going into my arm. My blood tests were all done and dusted in under ten minutes.

The speed at which private healthcare moves is incredible. I was sitting in the waiting room for under half an hour while Graham told me all about Manzies, the local pie and mash shop that still served jellied eels, before Dr Bhan called me back in. He had all of my blood results on his computer screen.
‘There’s definitely something going on with your white cell count,’ he said in a pacifying tone. ‘Your neutrophils and ESR markers are raised. Your red cell count, haemoglobin count, and mean corpuscular haemoglobin concentration are too high. I would just like to examine your masseter region again,’ he said. He stood up.
A Lightbulb Moment

Dr Bhan pressed into my jaw area with his thumb and middle finger. I squealed.
‘Is it painful there?’ he asked.
‘It’s agony, Dr Bhan,’ I said, ‘Please can you help me?’ A tear dropped from my eye and landed on his Jesus Creeper sandals, which he was wearing with socks.
‘I’m on your side,’ he said, holding my hand. ‘I think you may have some lymphatic drainage damage.’
I looked into his wide brown eyes and studied the small tufts of blackened hair around his ears. ‘What’s lymphatic drainage damage?’
‘Well…’ he began before clearing his throat. ‘Pervasive infections like this can sometimes damage the lymph nodes. This means that lymph fluid cannot drain away as it should, and this can create stubborn swelling and repeated infections.’
He just admitted that I had an infection. ‘What can we do about that?’ I asked.
‘I don’t know, Felisha, this is a challenging situation,’ he replied. He pronounced my name the American way. It grated a little, but I liked him too much to correct him. ‘It’s rare to have this condition in the facial region,’ he continued. ‘Most patients get lymphoedema in the arms and the legs.’
Empirical Treatment

We sat back down. I felt a weight lift off my shoulders. Someone was trying to help me. The midday sunlight was streaming into his consulting room. Dr. Bhan pulled out his prescription pad. ‘I can’t provide a diagnosis at this stage, but there is clearly something wrong. The blood tests show evidence that you have an infection, and your masseter area is tender, but I’m going to have to treat this empirically.’
I didn’t know what empirically meant, but I looked it up in the dictionary when I got home. Empirical treatment is the initiation of antibiotics before identifying what the infecting microorganism is. He was going to treat my illness with antibiotics without knowing the exact cause of my disease. Fine with me. He removed the cap from his beautiful black-and-gold fountain pen.
‘OK,’ I replied.
‘I don’t know are three of the most difficult words for a doctor to say. I’m afraid that I don’t know exactly what this is, but I’ll hang in with you until you’re better,’ Dr Bhan said.
I loved this guy. I didn’t love him in an inappropriate way, but instinctively and innocently. He was a deeply intelligent medic who had an enquiring mind and the ability to be honest and humble in a way I had never seen in a doctor before. We talked through different antibiotic options.
‘I’m going to try you on Rifampicin,’ he said. ‘It’s an antibiotic that treats tuberculosis, but it’s potent. It may help to alleviate your symptoms. I’ll give you two weeks’ worth of capsules and I’ll see you again in a fortnight. We’ll see how you are then.’
I watched as he wrote me a prescription. He had broad cursive handwriting. Dr Bhan handed me a pink private prescription and a blood test form. ‘I’d like you to get these blood tests done before I see you next,’ he said, and he walked me out of the department with his characteristic grace.
Relief

I made my way down to the hospital pharmacy. The Rifampicin cost £70.00. The blood tests cost £200.00, and the consultation with Dr Bhan was £195.00. The pharmacist handed me two boxes of antibiotics and warned me that my urine might turn darker while I was on them. I quickly swallowed two burgundy capsules with a cup of water that I got from the water cooler. I sat on the leather sofa opposite from where the dispensary, and I asked them if it would be OK for me to rest on the sofa for a few minutes.
‘Certainly, Madam.’
I must have laid down. My memory is hazy, so I can’t remember, but I woke up on the black leather sofa three hours later. It impressed me that the staff had left me to rest. I felt a deep relief, like I was just recovering from a burning fever. There was still that stubborn pain in my face, but the change in how I felt systemically was radical. I thanked them and left the hospital.
After I left the hospital, I wandered through Borough Market, enjoying the cheese stalls, the bright tulips, and the fresh fruit and vegetables for sale. The Asian aromas wafting from the Oriental food stalls reminded me of my travels to India. I found a cafe, where I bought a cuppa for £1.00. I drank my tea while listening to the rail squeal as trains drew into London Bridge. The relief that I felt from having taken those Rifampicin capsules was miraculous.


Waterloo

I walked towards Waterloo. The ambience was more vintage than I remembered. There were quirky bookshops and funky restaurants dotted around. It was early evening. The sky was still bright, and the temperature was warm. There were groups of people sitting outside drinking beer. I found a Persian restaurant, where men sat outside puffing on hookahs. I was starving. Because of feeling so nauseous, I hadn’t eaten properly for weeks. I ordered a kebab and flatbread, which I scoffed. The Middle Eastern taste of caraway seeds blended with turmeric was wonderful. Then I headed across the road to the Young Vic Theatre, where I bought a ticket to see a one-woman show. It felt like a celebration. I wasn’t better. Far from it. But I had found a doctor who ‘was on my side,’ and I finally had some medicine in my system.
Antibiotics & Steroids

I saw Dr Bhan every two weeks from May to October, 2014. After that, my appointments with him became monthly. The oral Rifampicin didn’t affect the pain and swelling in my face. The capsules did, however, alleviate those awful chills and my malaise. We cycled through different antibiotics, including fluroquinolones, Ciprofloxacin, and Levofloxacin. Unfortunately, Levofloxacin gave me severe Achilles tendonitis, which I still have after 9 years. Levaquin is a lethal drug, which I believe Janssen Pharmaceuticals stopped making in 2017.
We looked at the option of Dr Bhan prescribing Linezolid, the effective antibiotic that Professor Wong had prescribed, which is known to penetrate soft tissue and muscle better than other antibiotics. But a private prescription for one week of Linezolid was £1000. Back in 2014, Zyvox had the patent, and there was no generic brand. As a paying patient, that was out of the question.
Dr Bhan tried me on an eight-week course of oral Prednisolone with a reduced weekly dose, but the steroids made my symptoms worse. They produced a nasty feeling of pressure, like someone was pressing a heavy sheet of iron across my face. We didn’t try them again.
It was a difficult one. My neutrophils, red blood count (RBC), white blood count (WBC), and mean corpuscular haemoglobin concentration (MCHC) came down to within the normal range when I took the antibiotics. I felt less unwell systemically, and those nasty chills diminished. However, my facial pain only slightly mellowed. When I came off the antibiotics, my symptoms returned within days, and my infection markers shot up. There was no explanation for this, but I was certain that there was a stubborn infection going on in my facial soft tissue.
A Small Triumph

I felt the imprint of Professor’s Wong’s decision to terminate my treatment every time that I paid for my appointments with Dr Bhan. Each visit, including travel to and from London and an overnight stay in London, was around £590.00. This included the blood tests and medication. However, I was, thankfully, able to return to my Master’s degree in October 2014, thanks to Dr Bhan’s care. I had only missed one term. It was challenging to write with the persistent pain around my eye. I could only write for short bursts, and attending supervision meetings on campus took a lot of effort. I exerted that extra bit of effort because I was determined to carry on living my life in spite of my uncured illness.
Photo & Video Credits: Gustavo Fring, CottonBro Studio, Orlovamaria, Kampus, Ketut Subiyanto, Tonywuphotography and Alena Shekhovtcova on Pexels. Gerd Altmann, Kranich17 and Darko Stojanovic on Pixabay. Taras Chernus and Diego Ph and Michael Heise on Unsplash.

2024-08-27 01:25
London Calling
London Calling is an excerpt from my medical memoir. This is a work in progress. The genre is creative nonfiction. It is based on real-life events. All names have been changed to protect the identity of the individuals involved.
Chapter Four
February, 2014
London was calling. I was on the cusp of crisis. It was a mockery going to see the Loose Cannon’s colleague at the NHS Trust that he sent me to. His colleague followed his predecessors’ cause and wrote to my GP, ordering that my antibiotics be stopped. He did no blood tests either to see if my infection markers had normalised. ‘That’s your lot. No more medication. No more referrals,’ my GP said. I tried to move GP practice, but I was out of the ‘catchment area’ of neighbouring surgeries. I was screwed.

After the week-long prescription of oral Linezolid (600mg) and Ciprofloxacin (500mg) that Professor Wong had given me, I quickly deteriorated. The Linezolid had eradicated that feeling of worms wriggling inside my lower eyelid, but I still had persistent pain around my upper eyelid. My cheek was burning. I felt weak and fatigued. Chills washed up and down my jaw area, and my neck became stiff. It was impossible to carry through on any task reliably.
I was into my second term of the second year of my Master’s Degree (MA) in Writing at Sheffield Hallam University, where I was writing my first book. I knew that I could not complete this course in my weakened state, so I negotiated with the university, who kindly granted me one term off. The countdown was on. I had 16 weeks to find a doctor who could get me well enough to resume my studies.
Fight or Flight

The pressure was on. I had to act quickly. On a misty morning in late February, 2014, I headed for the capital. I took an early morning train from Mytholmroyd to Kings Cross in the hope of finding a doctor who could help me. I knew that this was not going to be easy; two high-calibre oculoplastic surgeons in the north of England had both said that there was nothing wrong with me. It was unlikely that a new medic would undermine their opinion, but at least I was going down to London with my eyes wide open.

It was strange exiting Kings Cross station. This was my first time back in London since 2004. The busyness felt foreign, but the familiarity of my adolescent stomping ground quickly came alive as the number 46 and C11 buses whizzed by. These were routes that I used to take to and from home – a home that was no longer there. Mum died in 2012, so my childhood home had been emptied. I had severed ties with my family in 2004, so I was now a visitor in my hometown. There was a cocktail of both sadness and liberation in my heart. I had no reference point anymore in London, yet I was free of the pain of those family relationships and could explore London on my own terms. I could only wish them all well and put my best foot forward. Which is what I did.
Harley Street

I checked into a hotel near Baker Street, not far from where my auntie Alexa had lived. Memories of eating smoked salmon and cucumber sandwiches at her and Uncle Isidor’s on Saturday afternoon’s hit me in a wave of nostalgia. I spent two weeks consulting with oculoplastic surgeons on Harley Street. It wasn’t cheap at £250.00 a pop, and I squandered a quarter of my share of my mother’s estate seeing these ageing men in Georgian houses. I got a blood test done privately, and my neutrophil and infection markers were still raised. Why had they terminated my treatment when I clearly still had an infection? The injustice felt hard to carry. I didn’t get anywhere on Harley Street. When these ophthalmologists learnt that I had been under the care of Professor Wong, their interest in looking at the problem with fresh eyes quickly diminished.
My MP

I had written to my MP before I set off for London. He agreed to see me at the Houses of Parliament. Once through the revolving doors, a member of staff handed me a visitor lanyard, and my MP greeted me with a firm handshake and kind manner. He was suited in pristine attire and wore spectacles that were tinted like shades. He bought me a frothy latte in the busy canteen, which was south of the foyer and full of official-looking people chatting. My MP asked me how he could help. I told him that they had stopped my medical treatment up north and that I was in a lot of pain. He said he wanted to phone my GP to get a clearer picture about what exactly was going on, and he asked me to give him a couple of days to do this.
My Father’s Legacy

After leaving The Houses of Parliament, I headed towards Parliament Square. I swerved left onto Little George Street and caught sight of the court where my father used to work. My father was a circuit judge and had sat at Middlesex Guildhall for most of his career. I found myself walking into the courthouse, hungry for familiarity and connection. A security guard with a potent aroma of aftershave asked if he could help. I told him that my father had worked here and that I was curious to see the building. ‘Hang on a minute,’ he said, and he went over to converse with an older man, who was sitting behind a desk area made of grey stone. This second gentleman wore a pale green shirt with rolled up sleeves. His lips curved upwards in an open, friendly expression as he hobbled towards me.
‘How can I help?’ he asked.
I repeated my cause.
‘Who was your father?’ He gently enquired.
‘Judge Alan Peter Solomon,’ I replied, choking on an unexpected flow of tears.
‘I remember Judge Solomon. He sat in Courtroom Two,’ he said, radiating a warm smile. He proceeded to tell me an anecdote about my father. Often, when security officers would take a quick snooze on the stairs when the building was quiet, my father would give them a gentle kick in the shins as he came down the stairs. Wake up sonny. That made me laugh.
‘May I go and see his courtroom?’ I asked.
‘Certainly, Madam. Courtroom two is empty this afternoon. I’ll take you up. Sorry, I didn’t get your name.’
‘I’m Felicia. Felicia Solomon. My father’s second born.’
‘Follow me,’ he said, and he led me up a spiral staircase.
Courtroom

The kind man left me to sit quietly in my father’s courtroom. It was a beautiful room that had a church like silence about it, with magnificent stained-glass windows steeped in history. The red thronelike seat at the front was where my father would have sat. His power wasn’t something that I had conceived of before. I sat in the courtroom for two hours, drawing on my father’s fortitude. I recalled the things that he used to tell me as a young girl on those Sunday afternoons, when he took me to The Garrick Club for lunch. He would talk to me about justice and the importance of standing up for truth. Never be frightened to speak up to those in authority, he said. They are just people, like you and me.

I left the courthouse feeling strengthened and wondered through Deans Yard, along Tufton Street, back to the house where I spent the first four years of my life. 15 Lord North Street, a four-story Georgian house, with a black door and a brass knocker, just a stone’s throw from Parliament Square. The house hadn’t changed. Nor had St. John’s Smith Square at the end of the street. It was still as majestic as I remember it. I eyed up my childhood home, remembering the creaking stairway and funny basement room where my brothers had slept. The funnel of our destiny is strange. I began my life in wealthy beginnings but was now hotel hopping, pleading with men in power to believe me about my facial pain. Where was the twist in my biography?

A Hostel

My MP called me on my mobile two days later. He had spoken to the manager at my GP practice, who had told him that they would ‘refer me to a consultant if I found one in London, and if they agreed with their diagnosis.’ That was firmly putting the responsibility on my shoulders. It was clear communication that the burden to find medical help was on me.
My budget was fast dwindling, so I checked into a hostel above a pub in Pimlico. It was £12.00 per night, including breakfast, which was a homemade omelette and a cup of coffee. The dormitories had sweeping views of the River Thames but stank of body odour and cheesy feet. I was in a fourteen-bed mixed dorm, which was mainly occupied by 19 year-old Swedish girls who went out on the lash until 2.00 am. It was impossible to get any rest, but I bagged a lower bunk bed by the window, which I insisted was left open for air. At least I had the view of the pretty lights along the Chelsea and Albert Bridges to look at at night.

My face continued to swell and burn, which I nursed with a cold flannel. I became more anxious as the weeks went by with no result. My facial pain was worsening by the day, as was the barricade that I was facing from the medical fraternity. I consulted with an infectious diseases consultant on Wimpole Street, who, despite finding my ESR and infection markers raised, told me to ‘live with the pain.’ He was so vile that I didn’t pay the £250.00 invoice. He must have reflected on his arrogance, as he never pursued me for the money.
Family Estrangement

It was unnerving walking the streets of Pimlico. One of my now estranged siblings only lived meters from where I was staying, though I didn’t know if they lived there anymore. Riding the number 24 bus around the familiar streets of Victoria and Pimlico was strange, constantly reminding me of Christmases been and gone and those pained visits to my father at his nursing home in St George’s Square, where his life ended in 2001. Family estrangement is hard to grapple with. There will always be fond memories of loving moments with estranged relatives, but when one has severed ties for serious reasons, those reasons must not be forgotten.
A Mini Breakthrough

I finally crossed a hurdle in April 2014, when I consulted with an oculoplastic surgeon at a private hospital in St Albans. He was a charming Arabian man who was willing to think more independently than the Harley Street boys. Mr. Badawi wore a pressed navy suit and had tight black curls crowning his head. He had a regal aura and a commanding voice. He did a punch biopsy of my eyelid tissue, which came back chronically inflamed, along with some blood tests, which showed further evidence of infection.
‘You need a physician,’ he said. ‘I think you have a systemic problem.’
I told him how unwell I felt and how bad my periocular pain was, but he said that he couldn’t prescribe medication without knowing what he was treating. He referred me to a physician at a private hospital in South London and to a Professor of Ophthalmology at a London NHS Teaching Hospital, who specialised in inflammatory eye conditions. He advised that my GP would also need to refer me to the professor because I would be seeing him on the NHS. I was grateful for Mr. Badawi’s care, and I was confident that his referrals would lead to some kind of help.

Heading Home

I had not had any medication for three months. I felt malaise and weak. The pain in my cheek and eye was stubborn and penetrating, and I was losing heart about returning to my Master’s Degree. I kept in touch with my MA supervisor by phone, who encouraged me to keep writing and get back to college as soon as I could. Within a week of Mr. Badawi making his referrals, I received an appointment to see this private physician on May 2nd, 2014, at 11 a.m. I was delighted. I packed up my belongings and said goodbye to my hostel. It had been an exhausting couple of months, and I had racked up a bill, so far, of £5900.
I headed back up north to my home in Calderdale and waited two very long weeks before returning to London to see this new physician.
Start by doing what’s necessary; then do what’s possible; and suddenly you are doing the impossible.
Francis of Assisi

Recommended Articles & Videos
Literary Style and the Lessons of Memoir
Narrative Style: The Heart of Storytelling & Why it Also Matters in Memoir.
How I Wrote My Memoir; One Notecard at A Time
Photo Credits; Ksenia Chernaya, Pixabay and John Carlos Salazar on Pexels. Gordon Johnson and Falco on Pixabay. Martijin Baudoin, Andrei Ianovskii, Mariana Alves, Towfiqu Barbhuiya, Paul Silvan, Chino Rocha, Timo Stern, Who’s Denilo? Gilberto Olimpio and Monika Guzikowska on Unsplash.

2024-07-24 06:19
On Chronic Illness And Identity
Introduction
‘Chronic illness shatters our biography.’ These are the most poignant words that I have seen posted on social media since I joined X, (formerly Twitter.) Living with chronic illness changes us beyond measure. Most of our energy is spent coping with and managing pain. This slowly chips away at our identity and sense of who we are. This post discusses the ways in which chronic illness erodes our identity. It also explores how we can find positivity and meaning through our new identity, that emerges.

Our identity is who we are in our exterior selves; the part of ourselves that we project out to the world. Our identity can comprise of the job we do/our profession, our financial status, our marital status, the kind of home we live in, and the clothes we wear. Identity is the colour and texture of the bricks that make up our metaphoric house. Our identity is how people see us, and from which they form assumptions about our persona. This is why our identity feels like such a core part of who we are.
Loss & Grief

Grief is an inescapable part of living with chronic illness, (invisible illness or apparent) because there are many losses that we face. There is a loss to one’s quality of life; we cannot do the things that we used to enjoy doing. There is a loss of career for many. Some people cannot do the job that they used to do. With the loss of one’s vocation can come a loss of self-esteem. We are heavily defined by what ‘we do’ in the world, and with this loss of career can come a real splintering of our confidence.
Our self-worth collapses, as we question our value in society, to our family, friends, and even to ourselves.[1]
As we endure living with chronic illness, we can become less driven and ambitious, and with that can come an inability to see a future for ourselves. Living with chronic illness also involves the loss of relationships; some do not have the patience to stand by a person living with enduring pain, so some relationships can sadly die. All of these losses comprise the shattering of our identity.
Chronic Illness has gnawed away at my self-identity, self-esteem, and self-worth. A single diagnosis – antiphospholipid syndrome was an immediate confiscation of my sporty, tomboyish, tough girl persona.[2]
Self-Acceptance

It takes an enormous dose of self-compassion to allow oneself to grieve for the person we were before chronic illness made an appearance in our lives. We often associate grief with the death of a loved one, so it can feel indulgent to allow ourselves to grieve the loss of our identity. It was only on my fiftieth birthday, that I allowed myself to acknowledge that things have changed irreparably. I couldn’t even look at it before then. That moment was liberating, because the realisation brought with it a dose of self-acceptance. I am not the same as I was before my facial pain began, and that is OK. Finding self-acceptance can be tough, especially when we look and feel different to the person we once were. But with acceptance, comes relief and freedom.
There is a sense of peace that settles in your being, when you let things go and let things be [3]
A New Dawn

With every death comes a birth, and whilst chronic illness may steal our identity, a new one does slowly emerge. I can’t claim to have found my new identity. I am still coming to terms with the loss of who I was before my facial pain began in 2013. But I can recognise new qualities that I have inherited. These qualities are compassion and resilience.
Since my chronic illness began, I am not so dismissive of others, particularly those who are vulnerable. I write my blog at my local library. There are two men who use the library as a refuge. One is an alcoholic, the other visibly struggles with his relationship with himself and the world. Before suffering with a chronic illness, I would have dismissed these lads as rogues, but over the last six months, I have spent time getting to know them.
Patience & Compassion
One of the lads loves eighties music. In my breaks, we sit on the bench outside, and sing along to tunes on my Spotify playlist; mainly The Human League and Fine Young Cannibals. We talk. Many folks in the community dismiss him because he looks shabby, but under his reddened cheeks and his beer-smelling breath, I have found a deep thinking, kind person, who before becoming ill, I would never have spoken to. I am glad to be better able to find humanity in those whose true qualities are hidden under a rough exterior. It may be a subtle trait to have acquired, but this lad appreciates it. ‘I love you to bits, Phillip,’ he says. (He calls me Phillip, because he can’t say Felicia.)

Whilst my emerging identity may be more tired and less ambitious, these qualities of patience, compassion, and generosity towards others, are qualities that I am glad to have bequeathed. I also have a stronger alignment with my core values. Truth, integrity and kindness were always important to me, but now they are at the forefront of my value system. So, in the shedding of our former selves, we must look for the value in the new self that emerges, even if it is a quieter version of the person we once were.
Quaker Beliefs

These losses that comprise the shattering of our identity, are external. They are things that we place value on from the outside of who we are. Whilst not a devout worshipper or believer in God, I have found inspiration from Quaker beliefs over the years. ‘At the centre of the Quaker faith lies the concept of the inner light. This principle states that in every human soul, there is implanted a certain element of God’s own spirit and divine energy.’[4] The spiritual discipline of Quakerism allows for a place ‘of quiet where we clear our systems, and are more open to one another and to compassion for ourselves. Whilst there is a deep inner self, there is that of God in each of us. There is something bigger than me, some bigger reality, some reality that encompasses all of us.’[5]
I draw on these principles as an important reminder that our soul or spirit is still alive and intact, even if chronic illness shatters our identity. Our spirit is a never-ending source of strength to draw from, and even though our lives may have changed beyond measure externally, we can still find resource and inspiration internally.

A Chronic Voice

Photo; Sheryl Chan, Founder of A Chronic Voice.
Sheryl Chan is the founder and author of A chronic Voice, a website and blog that is dedicated to raising awareness about the multi-faceted dimensions of living with chronic illness. She is a highly respected voice in the chronic illness community. Sheryl wrote a blog post, entitled What Never-Ending Pain Reveals to You. Her post woke me up to the silver lining in the cloud of living with a chronic illness.
‘The biggest realisation that dawned on me,’ she says, ‘is how fragile human beings truly are. There is a subtle arrogance when one possesses a body that is free of ailments. You feel invincible; that as long as you have enough willpower, you can conquer the world. This arrogance becomes a norm that permeates into every aspect of our lives. When you live with never-ending chronic pain, you come face to face with your mortality on a daily basis. You realise how little it takes to break the human body; yet you also realise how much life there is in one single breath. Chronic pain forces me to examine my mortality such that I can live with more purpose.’[6]
Small Moments

Sheryl’s words hone in on the fact that whilst having a chronic illness accentuates one’s fragility, it also pushes us to find life in small moments. These moments may be as simple as appreciating orange roses in full bloom, enjoying the sound of a child laughing, or relishing the taste of a luscious Greek salad. Whilst these moments may not be glitzy, they are still meaningful, and they are available to us if we allow them to touch us. Illness can definitely push us to live with more purpose. Since I started my blog a year ago, I have written 60k words. So, fragile though we may now be, it is still possible to find meaning within our limitations.
Having a healthy sense of self is to understand that every human being has inherent value, no matter who they are, or where they come from.
Sheryl Chan; A Chronic Voice.

A Chinese Idiom

I want to end this post with the Chinese idiom for crisis. A Transpersonal psychotherapist taught me this idiom when I was in my early twenties. The idiom has two characters. The upper character means danger, and the lower one means opportunity, or a crucial inflection point when something begins to change.
The danger with chronic illness is that we give up. We stop trying. These dangers bring apathy, depression and a sense of alienation. Some with life-limiting illnesses do choose Euthanasia. Some end their lives themselves. All of these dangers have been lurking during my11-year period of living with facial pain. There have been weeks and months when I have come close to giving up, because living with acute pain has felt too hard. But every morning that I wake up, I try and push the compass towards opportunity. I ask myself, ‘where is the opportunity in this? What change point is possible for me?’
I haven’t found the answer. However, I am certain that there is an opportunity in chronic illness. Maybe it is about prioritising our values and finding purpose in an alternative way. Perhaps it is an opportunity to discover meaning in small moments and to become more compassionate towards ourselves and others. Finding the opportunity in chronic illness is an ongoing enquiry for me. I keep asking the question. Maybe you can to?
It is worth remembering that the greatest gain in terms of wisdom and inner strength is often that of greatest difficulty.
Dalai Lama

Foot Notes
[1] Chan S; Loss of Identity with Chronic Illness & The Plot Twist: Sharpened Self-Worth, June 13th, 2022, www.achronicvoice.com
[2] Quotation is taken from the same source as footnote 1.
[3] Quotation is taken from the same source as footnote 1.
[4] Weening H; Meeting the Spirit – An Introduction to Quaker Beliefs and Practices, 1995.
[5] Quaker Speak: Quaker Spiritual Disciplines, 2016.
[6] Chan S; What Never Ending Pain Reveals To You, October, 2016, www.achronicvoice.com

Photo Credits; Ansfoto, JaneB13, Congerdesign and Geralt on Pixabay. Dawid Zawila, Kazuend, Mike Labrum, Gordie Jackson and Giulia Bertelli on Unsplash. Pixabay and Miriam Espacio on Pexels. The photo of Sheryl Chan is copyrighted © to Sheryl Chan, 2024. It is not licensable. Sheryl granted me permission to use the photo for the purposes of this blog post only.

2024-07-08 09:36
On Medical Trauma
What is Medical Trauma?
Medical trauma refers to a ‘patient’s psychological and physiological response to a negative or traumatic experience in a medical setting. The experience may involve illness, injury, pain, invasive procedures, and distressing or dismissive medical treatment. Being treated poorly by healthcare providers can cause medical trauma, such as when medical staff are not attentive or sensitive to a patient’s needs. Poor communication can also increase a patient’s stress levels and lead to medical trauma.’[1]

Medical Trauma is often referred to as Medical PTSD, which is ‘simply saying that a post-traumatic stress response has occurred after a traumatic medical experience. Not being believed by doctors is one of the experiences that can lead to a post-traumatic response. When you experience pain, you need others to believe you and help you. If a medical professional is withholding belief, help, or not paying attention to your symptoms, it can lead you to feel helpless.’[2]
This post discusses my experiences of medical trauma over the last 11 years. It discusses the impact that medical trauma has had on my mental health and my ability to function. It also recounts how medical trauma has affected my ability to trust healthcare professionals.
My Medical Trauma

Over forty medical consultants have not taken my concerns about my facial pain symptoms seriously. Doctors not believing me is the direct cause of my medical trauma. Their dismissal of me has forced me to endure undiagnosed facial, periocular, ear, and head pain for 11 years. This has been exhausting and torturous. Consultants speaking to me in disrespectful ways, gaslighting me, and ignoring abnormal scans and blood test results when they know how much pain I am in have also contributed to my experiences of medical trauma.
I have had many deeply traumatic experiences. An ophthalmologist randomly terminated my medical treatment. Clinicians have committed to action plans. I then receive a letter from them, telling me that they have discharged me from their care. One head and neck surgeon ghosted for 18 weeks. I saw him once. He promised to do a scan and get me back to find a way forward but he didn’t contact me again. I have faced obscene mental health discrimination, which involved medical departments refusing to see me because of stigmatization. Some clinicians have not been honest about clinical findings, and most recently, my GP practice has falsified my medical records. These experiences have all contributed to my decade-long medical trauma.
Symptoms of Medical Trauma

The symptoms of medical trauma look similar to those of Post-Traumatic Stress Disorder, (PTSD) and include:
- Avoidance of stimuli- including doctors in this case.
- Emotional numbing.
- Exaggerated startle response.
- Persistent Fear.
- Flashbacks
- Hypervigilance; (being in a heightened state of alertness.)
- Anxiety
- Depression
- Insomnia
- Intense Emotions
- Intrusive Thoughts
- Social Withdrawal
- Feelings of rage or shame
- Skin Rashes [3]
My Trauma Symptoms

My trauma symptoms are synonymous with all of the above. Since February 2023, I have not felt able to attend any further consultations with clinicians. This is because the interactions with these professionals are too distressing. It even feels unnerving when I collect my repeat prescriptions from my local pharmacy. I am suffering from acute insomnia. I get on average 1-3 hours of sleep a night. At 2.00am most nights, I wake up because of facial pain and blind panic. I have regular flashbacks to consultations with surgeons, who have gaslighted and spoken aggressively to me.
My mood has been severely low for five years. The strain of events took their toll on me and I fell into a mental health crisis in October 2019. I feel furious towards the system that has chosen to leave me in pain and have also withdrawn socially as a result of my medical trauma. I feel shame about the way the medical establishment has treated me and I feel extremely vulnerable out in the world. Skin rashes have also been recurring on my arms.

My most pronounced symptoms of medical trauma are intense fear and hypervigilance. I feel afraid all of the time and am on hyperalert, wondering what these NHS bodies are going to do next.
One of medical traumas key distinguishing symptoms is hypervigilance, meaning you’re constantly watching for things. Hypervigilance also includes intrusive thoughts and nightmares. [4]
Bessel Van der Kolk on Trauma

In an interview with Story Box, Bessel Van der Kolk, author of; The Body Keeps the Score, defines trauma as an “Oh My God” experience. He says; ‘trauma is when you are confronted with something, and nothing prepares you for it, and you just get overwhelmed. You feel helpless, and you shut down. You become immobilised. Your whole system breaks down, and you don’t know where to turn anymore.’[5]
An ‘oh my god experience’ translates to me as a big shock moment. My medical trauma has consisted of repeated large-scale shock moments with medical professionals. These shocks occur frequently. Just as I come up for air from one shock, the next one happens. I get no respite from them. I am in a constant state of trepidation. Even now, as I write this post, I feel fearful about what nasty blow is coming next. I am still recovering from my recent discovery that my GP practice has deleted an entry from my medical record, which recorded me attending A&E for suicidal feelings on May 17th, 2024. Stupefied is the only way I can describe what I felt when I saw this.

These trauma experiences are like mini earthquakes. I feel shaken by scandalous incidents. These are instances where NHS agencies in power are failing in their responsibility to care for me. The ground beneath my feet never feels safe.
Help and Support
 Bessel Van der Kolk explains that what happens after trauma is critical. He says that ‘it is key to have people around us who are there to help and support us. A safe, stable, nurturing relationship is the only way trauma can heal.’ I have had and currently have no help or support from statutory services to deal with these medical traumas. Organisations and services that should be helping me have instead compounded my trauma.
Bessel Van der Kolk explains that what happens after trauma is critical. He says that ‘it is key to have people around us who are there to help and support us. A safe, stable, nurturing relationship is the only way trauma can heal.’ I have had and currently have no help or support from statutory services to deal with these medical traumas. Organisations and services that should be helping me have instead compounded my trauma.
Mental Health Services

The mental health services know that I am going through a prolonged trauma regarding my facial pain. Three teams have seen me in acute distress and despair. They know that I am not making up my facial pain. But they have either remained silent, blamed me, or colluded with the cover-up and protected the NHS bodies who have caused me harm.
A mental health team in Fife made matters much worse for me. A locum psychiatrist, who had never met nor spoken to me, wrote a letter that said that I have ‘Factitious Disorder.’ His letter said that I am making up my facial pain in order to ‘feed the need to have a sick role.’ He sent this letter to multiple agencies. As a result of this letter, I faced a wave of obscene discrimination: one surgeon ghosted me for 18 weeks, an infectious diseases clinician discharged me when my infection markers were high, and a pain management service refused to see me.
Blaming Me

My current mental health team, who have now discharged me, put the responsibility onto me. They told me that I need to ‘reframe’ the awful way that the medical system has treated me. They said that I don’t ‘like what I am hearing,’ and that I ‘need to hear some truths.’ This team was then complicit in the tampering of my medical records. I told them that my GP had written in my records: Scan abnormal to be expected; no action needed. Within two hours of telling that MH clinician, my GP practice locked me out of my System One portal and amended that record.
How do I ‘reframe’ that?
I attended Accident & Emergency on 10 June 2024 to get help for my suicidal thoughts. The psychiatric liaison officer who I saw said to me in a blunt way, You can’t come here for support. He then told me to ‘self-refer’ back to the statutory services who have discharged me and closed down my file. That was my ‘care plan.’ It beggars belief.
Social Services

The actions by social services have compounded my trauma. My local authority terminated my social care package in April 2023. They didn’t explain why. My previous authority, when I lived in Scotland behaved with even more brutality. NHS 111 raised 5 causes of concern to public protection. The local authority ignored them all. No one from public protection even called me for a welfare check. It’s not possible to turn to my GP for support, as their conduct has instilled deep mistrust and fear within me. I feel immobilised and helpless. The system has shut down on me. I find it difficult to tell people because it is so unbelievable. I have become quiet and withdrawn.
Trauma is very much about the whole system breaking down and you don’t know who to turn to anymore. It resets your orientation in the world.
Bessel Van Der Kolk
Fear & Hypervigilance

Bessel Van der Kolk advises that we have to pay attention to our feelings. ‘Our emotions,’ he says, ‘are warning signs. If you are anxious, our brain is warning us that something dangerous is happening.’ [6] My fear and hypervigilance are unrelenting. I feel fearful all of the time, even when I am doing day-to-day things, like buying a loaf of bread. However, when I read Bessel Van der Kolk’s words that say that fear is a warning sign, I am comforted to know that it is natural to feel afraid in the circumstances that I am in.
It is dangerous to be registered with a GP practice, who is tampering with my medical records. It feel terrifying to have so many government organisations colluding with one another and closing ranks in this vicious way. The imbalance of power feels so overwhelming.
Conclusion

My system has shut down, and I have become frozen with fear. I do not know where to turn anymore. I have no reference point within the healthcare system. No place of refuge. My medical trauma has made a significant imprint on me and has ‘reset my orientation in the world’ in a negative way. This incessant state of shock and hypervigilance that I am living with prevents me from being able to engage with people in the present moment and function normally.
These shocks that arise from harrowing interactions with medical professionals are still occurring, so I am on tenterhooks, wondering what they are going to do next. It’s not possible to start a recovery while the trauma is still alive. I cannot, therefore, begin to heal from these traumas until they stop happening. Once they cease, I hope that with the right help, these distressing experiences will thaw in my consciousness and gradually have less hold over me.
Fortunately, the vast majority of medical experiences are positive ones, sometimes with truly heroic efforts by doctors and nurses to save a patient’s life. But when things go wrong, it can be emotionally devastating.[7]

Foot Notes
[1] Blanchfield T, (AMFT) What is Medical Trauma? 31st January, 2022, www.verywellmind.com
[2] Dr Quincee Gideon; Common Symptoms of Medical PTSD, www.woventraumatherapy.com
[3] Information quoted from same source as footnote 1.
[4] Goldman, L: What You Need to Know About Medical Trauma, April 19th, 2021, www.healthcentral.com
[5] Bessel Van Der Kolk; The Body Keeps the Score| Understanding & Healing from Trauma, The Story Box.
[6] Quotation taken from same source as footnote 5.
[7] Goldman L; What you Need to Know About Medical Trauma, April 19th, 2021, www.healthcentral.com
Recommended Articles
Medical Trauma: Signs, Causes and Care
What Does Emotional Trauma Look Like?
Videos on Trauma
Photo Credits; Bansah Photography & Savannah on Unsplash. Andrea Piacquadio, Engin Akyhurt & Alexander Krivitskiy on Pexels. Gerd Altmann, Tiro Prasetyo, Public Domain Pictures, Anemone123 & Alexas Fotos on Pixabay.

2024-06-29 06:59
On The Falsifying of My Medical Records #2
This blog post contains wording about suicide that some people may find triggering. If your need is urgent, please call 999, (UK) . If you need support, please call 111, (option 2) or call The Samaritans, freephone helpline;116 123.
Introduction
The Falsifying of my Medical Records #2, follows on from my previous post, in which I recounted five serious incidents where my GP practice amended, deleted, falsified and omitted data from my medical records. They amended one record 18 months after the date that they made the initial entry, without being transparent about why. The GP practice has deleted one record, which documented me attending Accident & Emergency, (A&E) for suicidal thoughts, and a GP partner, who has never met or spoken to me, falsely recorded that she did two ‘interim depression reviews’ with me. They also deleted and then re-entered a record six weeks after they first entered the record, and did not record that I called 111 for suicidal thoughts.

This post discusses the falsifying of my medical records within the context of The Data Protection Act, 2018, and Article 5 of The UK General Data Protection Regulation, (GDPR,) which ‘makes provision about the Information Commissioner.’[1] This post also examines these incidents within the framework of the ‘False and Misleading Information offence,’ (FOMI.) It calls for urgent legal assistance, to help me out of this perilous situation.
The Data Protection Act 2018

The Data Protection Act 2018 controls how your personal information is used by organisations, businesses or the government. It is the UK’s implementation of the General Data Protection Regulation (GDPR). Everyone responsible for using personal data has to follow strict rules called ‘data protection principles.’ They must make sure the information is:
- used fairly, lawfully and transparently
- used for specified, explicit purposes
- used in a way that is adequate, relevant and limited to only what is necessary
- accurate
- handled in a way that ensures appropriate security, including protection against unlawful or unauthorised processing, access, loss, destruction or damage. [2]
The Data Protection Principles

Relevant to the falsifying of my medical records, Article 5 of the UK GDPR requires that personal data be;
(a)Processed lawfully, fairly and in a transparent manner in relation to individuals (‘lawfulness, fairness and transparency.’)
(b)Collected for specific, explicit and legitimate purposes. (‘Purpose limitation.’)
(d)Accurate and kept up to date. (‘Accuracy.’)
(f)Processed in a manner that ensures appropriate security of the personal data, including protection against unauthorised or unlawful processing and against accidental loss, destruction or damage. (‘Integrity’ & ‘Accountability.’) [3]
Article 5 (2) adds that; The controller shall be responsible for, and be able to demonstrate compliance with these principles. Article 83(5)(a) states that infringements of the basic principles for processing personal data are subject to the highest tier of administrative fines. [4]
A Closer Look at The GDPR Principles

(a): Lawfulness, fairness and transparency means that the controller of data and information;
- must ensure that you do not do anything with the data in breach of any other laws.
- must use personal data in a way that is fair. This means you must not process the data in a way that is unduly detrimental, unexpected or misleading to the individuals concerned.
- must be clear, open and honest with people about how you will use their personal data. [5]
(d): Accuracy;
- Take all reasonable steps to ensure the personal data you hold is not incorrect or misleading as to any matter of fact.
- If you discover that personal data is incorrect or misleading, you must take reasonable steps to correct or erase it as soon as possible.
- You must carefully consider any challenges to the accuracy of personal data. [6]
(f): Integrity and Confidentiality, security;
This principle states that the controller; must ensure have appropriate security measures in place to protect the personal data you hold.[7]
Accountability;
The accountability principle requires the controller to take responsibility for what you do with personal data and how you comply with the other principles. You must have appropriate measures and records in place to be able to demonstrate your compliance. [8]

Data Protection- Criminal Offences
The information that is available on The Crown Prosecution Service’ website, shows that it is a criminal offence to destroy or falsify information, (section 148) and to ‘re-identify’ data that has been ‘de-identified,’ (section 171.) Under Section 148 (2) (a) it is an offence for a person to destroy or otherwise dispose of, conceal, block or (where relevant) falsify all or part of the information, document, equipment or material.[9]
Section 171 is a new offence- it criminalises the re-identification of personal data that has been ‘de-identified’ (de-identification being a process-such as redactions-to remove/conceal personal data). Section (5) states that it is an offence for a person knowingly or recklessly to process personal data that is information that has been re-identified. Sections (3) and (4) set out the defences to section 171 (1) – for example, the re-identification was necessary for the purposes of preventing or detecting crime. [10]
Reflection

My GP practice has broken the law by falsifying my medical records. They have breached 3 principles of Article 5 of GDPR. They have breached; principle (a) Lawfulness, fairness and transparency, principle (d) accuracy, and principle (f) integrity, confidentiality and accountability. The practice has committed a criminal offence by destroying the entry on my records, which recorded that I went to A&E on May 17th for suicidal thoughts. They have also not been accurate by not recording that I phoned 111 on 22nd July, 2024.
They have breached the law by falsifying two entries that stated that the GP partner did two depression reviews with me, (section 148; destroying or falsifying information and documents etc.) If the GP practice now ‘re-enact’ the information that they have ‘de-enacted,’ then they are committing another criminal offence, (section 171: Re-identification of de-identified personal data.) Their recent re-identifying of the de-identified data from 10th June is a criminal breach of section 171. They should not have re-entered the first entry from 10th June that they deleted.
The Rights of Data Subjects

I am alarmed about the falsifying of my medical records. I am particularly concerned about the data that the GP practice has omitted from my records. Due to the number of NHS bodies involved in this cover-up, I don’t feel able to challenge the GP practice myself about their conduct. I need legal help. However, I am comforted to know that the GDPR provides data subjects; 1) the right to object, 2) the right to restrict processing and 3) the right to rectification. I should, therefore, be able to my records put right. I would hope to be able to get the falsified entries removed and the deleted record, which documented me attending A&E on May 17th, 2024 for suicidal thoughts, put back onto my records, (rectified.) [11]
The False or Misleading Information Offence, (FOMI.)

Following the Mid-Staffordshire inquiry, when Mid Staffordshire Hospitals tried to hide that there were problems, it became part of The Care Bill that it was a crime for Health and Social Care providers to publish false or misleading information. The Care Act, 2014 ‘put in place a new criminal offence applicable to care providers who supply or publish information that is false or misleading, where that information is required to comply with legal obligation,’ (1.) This was part of the coalition government’s drive to improve openness and transparency in the provision of health services. The offence is in two parts; 1) It is a ‘strict liability offence where a provider is found to have published or provided false or misleading information, and 2) where a ‘director or senior official are found to be culpable in the offence,’ (6.) [12]
To be clear, re the definitions of false and misleading. ‘False information is that which can be demonstrably proved to be incorrect’ (11.) ‘Misleading information is presented in such a way, that the meaning is distorted. The information must mislead the intended audience in some way,’ (12.)[13]
Who Does FOMI Offence Apply to?
The False or Misleading Information Offence: Guidance for Providers states that; (14) The offence can be committed by a “care provider of a specific description.” “Care Provider” means a public body which provides health services or adult social care in England. Fact Sheet 14 states that; ‘initially regulations will limit the criminal offence to providers of NHS secondary care.’[14]However, clause (522) of The Care Act 2014- Explanatory Notes- False and Misleading Information, states that; ‘The offence thus applies to public bodies that provide health services or adult social care in England, such as NHS Trusts, NHS Foundation Trusts and local authorities; and to all types of GP practice, whether sole practitioners or partnerships (and whether they have entered into personal medical service or general medical service contracts with NHS England,) (522.) [15]
Reflection

Whilst ‘False or Misleading Information,’ (FOMI) applies, in the main to NHS secondary care, General Practitioners, (GP’s) are still expected to adhere to accurate and transparent information practices to maintain patient trust and safety. For a GP to enter onto a patients’ record that she has conducted two depression reviews, when she has never met or spoken to the patient, is false and misleading information. It is false because it is incorrect. It is misleading because it looks like the GP has been giving the patient support, when they have not.
Conclusion

This post has framed the falsifying of my medical records within the context of The Data Protection Act, 2018 and FOMI. My GP practice has breached these laws by deleting data and falsifying entries on my records. I am in a very vulnerable predicament, and feel very afraid. I am not in the hands of safe healthcare providers. This is dangerous misconduct, that is putting me at risk. I need the assistance of a lawyer, who can help me out of this situation. I am also seeking a medical journalist, who can bring my story to the attention of the public eye. If you think you can help, please get in touch by email; info@myfacialpain.com, via my contact page or @myfacialpain on X.

Foot Notes
[1] Data Protection Act, 2018, Part 1, Section 1, www.legislation.gov.uk
[2] Data Protection: The Data Protection Act – GOV.UK (www.gov.uk)
[3] Information Commissioner’s Office; A guide to the Data Protection Principles, www.ico.org.uk
[4] Information Commissioner’s Office; A Guide to the Data Protection Principles, www.ico.org.uk
[5] Information Commissioner’s Office; Principle (a): Lawfulness, Fairness and Transparency, Data Protection Principles, www.ico.org.uk
[6] Information Commissioner’s Office: Principle (d) Accuracy, Data Protection Principles, www.ico.org.uk
[7] Information Commissioner’s Office: Principle (f) Integrity and Confidentiality (security,) Data Protection Principles, www.ico.org.uk
[8] Information Commissioner’s Office; Principle: Accountability, Data Protection Principles, www.ico.org.uk
[9] The Crown Prosecution Service (CPS); Offences Under the DPA 2018, Data Protection Act 2018 – Criminal Offences, www.cps.gov.uk
[10] The Crown Prosecution Service (CPS); Offences Under the DPA 2018, Data Protection Act 2018 – Criminal Offences, www.cps.gov.uk
[11] GDPR Summary; Data Subject Rights: All You Need to Know, www.gdprsummary.com
[12] Department of Health; The False or Misleading Offence: Guidance for Providers., www.publishing.service.gov.uk
[13] Information quoted from same source as footnote 12.
[14] Department of Health; The Care Bill – False or Misleading Information, December, 2013.
[15] The Care Act 2014 Explanatory Notes, part 2, False or Misleading Information, www.legislation.gov.uk

Photo Credits; Ferarcosn, RDNE Stock Project and Pixabay on Pexels. Emiliano Vittoriosi and Towfiqu Barbhuiya on Unsplash. Fathromi Ramdlon, Tho-Ge, Niekverlaan, Artsy Solomon, Leroy Skalstad and Bilijana Jovanovic on Piaxabay.

2024-06-29 06:55
On The Falsifying of My Medical Records #1
This blog post contains wording about suicide that some people may find triggering. If you are in the UK, and your need is urgent, please call 999. If you need support, please call 111, (option 2) or The Samaritans, freephone helpline; 116123.
Introduction
‘The act of falsifying medical records refers to the deliberate act of altering, changing or omitting a patients’ health-related documentation with the intent to deceive or mislead.’[1] ‘Falsification and tampering come in many forms; removing a diagnostic report, inserting information without standard documentation, destroying the record, and omitting significant facts. Often it is an attempt at damage control for a known error or an adverse medical outcome.’[2]

This post recounts the falsifying of my medical records by my GP practice. This has happened on four separate occasions. My discoveries regarding the falsifying my medical records are recent, and I am still in a state of acute shock. I have never experienced anything as alarming as this before. I am writing this post in the hope that by recounting these incidents, self-regulating healthcare practitioners will one day, not be allowed to do what my GP practice has recently done. Not without watchful scrutiny.
Incident 1; Altering

The first incident relates to my GP practice altering an entry on my records. I recounted this in This is A Cover Up. In July, 2022, I had an MRI neck scan, which showed abnormality. I saw that my GP had written; Scan abnormal, to be expected, No Further Action, in my records. On 8th December, 2023, 18 months later, I told a clinician from the Mental Health team, that I had seen my GP’s comment in my medical records, and that I was saddened by it.
That same day, my GP practice locked me out of my System One portal. They changed my password without telling me. On 11 December, 2023, when I requested a new password, I saw that the GP practice had amended that record. They had inserted; No Review Applicable to the entry, as highlighted below.

They did not indicate anywhere when they amended this entry, who did it and why. When retrospectively adding notes to the patient’s record, the record should include (in a way that is immediately apparent to an objective reader):
- The name of the person adding the information.
- The time and date of the addition.
- An explanation of which information has been added.
- An explanation of why these were not recorded at the time of the original entry and why they are being entered now.
‘Retrospectively amending patient records without an appropriate explanation in a non-transparent way, especially when it has been done so in a self-serving way, has serious implications that could result in criminal action, withdrawal of indemnity, or a GMC sanction.’ [3]
Context to Next Incidents

The strain of enduring facial pain for this long, as well as the blockade that the healthcare system has erected to me accessing treatment for my pain, has pushed me into a suicidal crisis. I have been dealing with this crisis since October, 2019. I had no previous episodes of suicidal ideation before this date. It is a direct result of dealing with unrelenting pain, and the way I have been treated by the healthcare system. I have had to present at Accident & Emergency (A&E) on a number of occasions, re my suicidal thoughts. When a patient has attended an A&E department, the hospital sends an electronic discharge summary to the GP, who then updates the patient record.
Incident 2; Deleting

On May 17th, 2024, I attended an A&E department for help with my suicidal feelings. I saw two liaison officers, who sent a letter to my GP and MH team, (who have discharged me.) The GP practice logged my visit to A&E onto my records. The record said;
17th May, 2024; Suicidal Thoughts (1BD1) (Ongoing Episode.)
17th May 2024; Seen in Accident and Emergency Department (9N19)
On June 7th, 2024, when I logged into my System One portal to request some cream, I saw that the practice had deleted the entry from May 17th, 2024. It was no longer there. I was dumbstruck. I didn’t take a photo of the original entry, but A&E provided me with the electronic discharge summary that they sent to my GP after my visit on May 17th. There is no log of this visit on my medical record. They have deleted it. As I do not have my paper records, I don’t know if the practice has also destroyed the letter that the liaison team sent to the practice. If they omitted record of me attending A&E, it is possible that they have destroyed this correspondence too.

This is the Electronic Discharge summary that A&E sent to my GP practice, after I attended on 17th May, 2024.

My casualty card from A&E on 17th May, 2024.

The red arrow shows where the record was that I attended A&E on 17th May for suicidal thoughts, that the GP practice has deleted.
Incident 3; Falsifying
On March 29th, 2023, I attended A&E for low mood and suicidal thoughts. The GP practice logged this onto my records;
29th March, 2023; Depressed Mood (XEO re) (Ongoing episode.)
29th March, 2023; Seen at Accident and Emergency (9N19.)
29th March, 2023: Suicidal Thoughts. (1BD1) (Ongoing Episode.)
One of the GP partners at the practice, who I have never met or spoken to, has falsely entered onto my records, that on March 23rd and March 31st, 2023, (either side of my A&E visit) she did ‘interim depression reviews.’ She did not conduct these depression reviews. I don’t know who she is. I do not take any psychiatric medication, so she could not have done a review by paper either. On March 31st, when she falsely entered that she did a ‘depression review,’ it looks like she retrospectively entered the ‘depression review’, that she falsely claims to have done on 23rd March.

Red arrow shows the falsified record made by the GP partner, who I have never met or spoken to, who entered that she did a depression review, 2 days after I attended A&E for suicidal thoughts.

Red arrows show the second falsified record made by the same doctor, who entered she also did a depression review 6 days before I attended A&E.
New Incidents
Incident 4; Deleting Data.
I am updating this post with 2 further incidents re; my GP practice falsifying my medical records, that have both happened since I published this blog post on 29th June, 2024. These new incidents refer to deleting, re-entering and omitting records. On 10th June, 2024, I attended Accident and Emergency (A&E) for suicidal thoughts. My intensified suicidal ideation was triggered after incident 2, (recorded above.) I was in a very bad way after this. The secretary at the GP practice, recorded my visit to A&E on 10th June, with 2 entries.
Entry 1 said;
10 June, 2024; Suicidal Thoughts (1BD1) (Ongoing Episode.)
10 June, 2024; Seen in Accident and Emergency, (9N19)
Entry 2 said;
10 June, 2024; Suicidal Thoughts, (1BD1) (Ongoing Episode.)
10 June, 2024; Mental Health Assessment, (Xa1YN) (Ongoing Episode.)

This is how the records looked on 15th June, 2024.
On Monday July 22nd, 2024, I logged into my System One portal to see if the GP practice had prescribed medication for a rash on my right hand. I saw that they had deleted the first entry from 10th June, 2024, which recorded that I was seen at Accident and Emergency. This is how the entry looked on 22nd July, 2024.

This is how the record looked on 22nd July.
Today, 26th July, 2024, when I logged into my System One portal, I saw that the GP practice has reinserted the first entry from 10th June, which they must have re-entered between the dates of 22/07/24 – 26/07/24. There are no notes to explain why one entry was deleted and then put back. This is how the record looks today. This photo was taken on 26th July, 2024.

Incident 5; Omitting Data

I had to call 111 on July 22nd, 2024 at 2.46am for suicidal thoughts. The First Response handler triaged me as needing to speak to crisis support urgently. She put me through to a mental health practitioner, who I spoke with for one hour in the early hours of the morning. The GP practice have not recorded my call to 111 on 22nd July, on my medical records.

Red arrow shows that GP practice have made no record of me calling 111 on 22nd July, 2024.
This is very sinister. I think it is the female GP partner, (who owns the practice) who is deleting these records. It is she, who falsely entered that she did two depression reviews with me in 2023, (incident 3.) It seems that the admin team are desperately trying to correct the falsifying of my records with the best intentions, and may explain why they re-identified the deleted first entry from 10th June, 2024. I am certain that if someone did an audit trail of my records, they would find that it is the GP partner who has deleted and falsified my records.
On July 3rd, 2024, I spoke out on X, (formerly Twitter) about the GP deleting the record on 17th May, 2024. That same day, the practice added an admin note to my record, which I think corresponds to that issue.

Administration note that GP practice added to my record on 3rd July, when I spoke out on social media about incident 2.
Falsification of medical records can compromise patient safety and break trust. It may also lead to inappropriate treatment, delayed or incorrect diagnoses, and potentially fatal medical errors. Not to mention that it’s illegal.[4]
Good Medical Practice

The GMC states that a registered medical practitioner is required to;
Record your work accurately
69 You must make sure that formal records of your work (including patients’ records) are clear, accurate, contemporaneous and legible. (Contemporaneous means making records at the same time as the events you are recording, or as soon as possible afterwards.)
Act with honesty and integrity
81 You must make sure that your conduct justifies patients’ trust in you and the public’s trust in your profession.
Communicating as a Medical Professional
88 You must be honest and trustworthy, in all your professional written, verbal and digital communications.
89 You must make sure any information you communicate as a medical professional is accurate, not false or misleading. This means:
a. you must take reasonable steps to check the information is accurate
b. you must not deliberately leave out relevant information
c. you must not minimise or trivialise risks of harm[5]
Reflection

These incidents of falsifying my medical records are a disgraceful breach of Good Medical Practice. Amending a record 18 months after the original entry was made, is not contemporaneous, (69.) Nor is it contemporaneous to delete and then re-enter a record six weeks after the record was entered. Claiming to have done two depression reviews with a patient who you have never met or spoken to, is not honest, (88). It is false and misleading, (89.) Deleting and omitting entries that record a patient attending A&E and phoning 111 for suicidal thoughts is trivialising risk of harm and putting a patient at grave risk of harm. The GP practice’ conduct neither justifies patients’ trust in them or the public’s trust in the profession, (81.) How can a patient trust a GP practice, who has a history of altering medical records?
The NHS Constitution for England

The NHS Constitution states that the NHS is ‘there to improve our health and well-being. It touches our lives at times of basic human need, when care and compassion are what matter most.’ It’s a beautiful document, but each time that I read it, I feel sad. This is because of how far removed the conduct of these clinicians is, from the values listed below, that the NHS Constitution upholds;
- Working together for patients
- Respect and dignity
- Commitment to quality of care
- Compassion
- Improving lives
- Everyone counts.[6]
Respect and Dignity

The NHS Constitution says;
Every individual who comes into contact with the NHS should always be treated with respect and dignity. This value seeks to ensure that organisations treat people as individuals, valuing and respecting different needs, aspirations and priorities. The NHS aims to foster a spirit of candour and a culture of humility, openness and honesty, where staff communicate clearly and openly with patients.[7]
Compassion

The NHS Constitution says;
Compassionate care ties closely with respect and dignity in that individual patients must be treated with sensitivity and kindness. The business of the NHS extends beyond providing clinical care and includes alleviating pain and distress and ensuring people feel valued and that their concerns are important.[8]
Reflection

When I saw that the GP practice had falsified and omitted these entries from my medical records, I felt sick with shock. I did not feel like they had treated me with respect and dignity. Quite the opposite. I felt dehumanised. This was not compassionate care. Their conduct felt violent, like they were eradicating any trace of my feelings or of my reality. How can an NHS body destroy medical data about the health of a patient, who they know is this worn down, just to protect another NHS service?
Final Reflection

The falsifying of my medical records is a breach of GMC guidance and a betrayal of the values of the NHS Constitution of England. The impact of my GP’s actions on me has been profound. I am shaken and demoralised, and I am extremely concerned about the data that the practice has deleted from my record. It needs reminding that there is a human life at the heart of this story. A human being who is simply seeking answers about her facial pain, and seeking support for the crisis that has ensued from the lack of treatment for that pain.
In; On Good Medical Practice #3, I ask if self-regulation of doctors works. No, it doesn’t. Not if doctors can falsify medical records like this, without regulation or accountability. I struggle to understand how it is possible for a GP to delete an entry from a patient’s record, amend an entry, and add false information without it being noticed. Conduct like this should not be able to go unregulated in healthcare. Reform is urgently needed so that perilous behaviour like this, which puts patients at grave risk of harm, is prohibited.
Patients must be able to trust medical professionals with their lives and health, and medical professionals must be able to trust each other.[9]

In the summer of 2023, there was a serious incident at my GP practice, that hit the UK headlines. In light of this, and my recent experiences that I have recounted here, I am concerned about the potential welfare of other vulnerable patients. I worry about how many other patients they are doing this to. Something is wrong, and it needs flagging.
Foot Notes
[1] The Dangers of Falsifying Medical Records; A Deep Dive, www.ifaxapp.com
[2] Falsifying Medical Records and Identifying Missing or Misleading Information, Medlaw Advisory Partners, Feb 27, 2021, www.medlawadvisory.com
[3] Amending Medical Records-Appropriate Circumstances and How It Should Be Done, February, 2022, www.lmc.org.uk
[4] Information quoted from same source as footnote 1.
[5] The General Medical Council; Good Medical Practice, 2023. This guidance came into effect o 30 January, 2024. www.gmc-uk.org/guidance
[6] Department of Health & Social Care; Guidance; Handbook to The NHS Constitution for England, October, 2023, www.gov.uk
[7] Information quoted from same source as footnote 6. www.gov.uk
[8] Information taken from same source as footnote 6 & 7
[9] The General Medical Council; Good Medical Practice, 2023. This guidance came into effect on 30th January, 2024.
Photo Credits; Carlos De Toro, Usman Yousaf, Onur Binay and Artem Kovalev on unsplash. Pixabay and Marlon Retratos on Pexels. Who_Made_This, Gerd Altmann and unknown on Pixabay.

2024-06-06 11:11
On Occipital Neuralgia
Summary
‘Occipital Neuralgia is a condition in which the occipital nerves, the nerves that run through the scalp, are injured or inflamed. This causes headaches that feel like severe piercing, throbbing or shock-like pain in the neck, back of the head and behind the ears.’[1] Occipital Neuralgia can be caused by trauma or compression to the occipital nerves, muscle tightness, or prior injury to the scalp or skull. It ‘can also be caused by underlying health conditions, such as arthritis, gout, and infection or inflammation.’[2] I am trying to find out whether peripheral damage or inflammation to my occipital nerves or blood vessels could be causing my head pain. This post asks whether my left-sided head pain, could be Occipital Neuralgia.

Symptoms

Symptoms of Occipital Neuralgia include a sharp, shooting, throbbing or burning pain in your scalp, neck, and behind your ear. ‘Pain that radiates to one side of your head, pain behind your eye, and sensitivity of your scalp,’[3] are also symptoms of Occipital Neuralgia. My symptoms have been getting progressively more severe. They include a piercing, throbbing pain behind my left ear, and it feels like someone is screwing a corkscrew into the top of my head. It also feels like there is a sheet of mist under my skin. This fog like feeling is all the way around the left side of my head. The pain is debilitating and unrelenting.

As previously explained, I also have persistent pain around and behind my left eye. From the bone behind my left ear, all the way up to the top of my skull, I experience an incessant burning pain. The region at the top of my head is the most painful. The pulsating pain there is acute. I am concerned.
Infection and Inflammation

Infection and inflammation are one of the secondary, underlying causes of Occipital Neuralgia. I have repeatedly indicated, that whilst medics have not identified an aetiology, infection and inflammation remain the two most likely causes of my condition. This raises the question, as to whether my occipital nerves could be inflamed or damaged, as a result of 11-yrs of chronic infection and inflammation in my fascial spaces. Could my head pain be related to inflamed nerves and blood vessels? Could Occipital Neuralgia be causing my left-sided head pain?
Conclusion
I have raised the issue of my left-sided head pain with many Ear, Nose and Throat (ENT) consultants. None of them have given me any answers or help. The oral antibiotics that I take, do quell my head pain, particularly Doxycycline, but they only give me temporary relief. I am seeking the help and advice of either a skull-based otolaryngologist or a neuro-surgeon, who can identify what is causing my head pain, and help to relieve it.
I have previously asked whether my left-sided head pain could be related to my mastoid, or to an enlarged temporal bone. The last ENT consultant, who I saw in 2022, mentioned both of these as possible causes of my head pain. I’ve also asked if the pain in my left temple area could be Temporal Arteritis. However, in the absence of any answers, my questions continue. Could inflamed occipital nerves and blood vessels be the cause of my left-sided head pain? Is Occipital Neuralgia the cause? If it is, how can medics treat this?

My Contact Details
If you think you can help, please get in touch. I would love to hear from you. You can contact me via the contact form on my website or directly by email; info@myfacialpain.com. You can also find me on X @myfacialpain.

Foot Notes
[1] Pilitsis J G, MD et al; Occipital Neuralgia, The American Association of Neurological Surgeons.
[2] Catanese L; Occipital Neuralgia: Symptoms and Treatments, Harvard Health Publishing, Harvard Medical School, March, 2024.
[3] Meyler Z; Occipital Neuralgia: What it is and How To Treat It, www.spine-health.com
Photo Credits; Imo Wegmann, Ira Pavlyukovich and The National Institute of Allergy and Infectious Diseases on Unsplash. Vie Studio on Pexels.

2024-05-29 08:23
On The Culture of Blame
Introduction
‘On the Culture of Blame’ concludes my recent series of posts on the NHS Complaints Procedure and the medical litigation culture. In those posts, I explored how clinicians rarely handle medical errors with candour, because of a defensive culture that exists within the medical landscape. I discussed how clinicians often cover for their errors, rather than own their failings and learn from their mistakes. This post attempts to understand the reason for this lack of accountability in medicine, which is the culture of blame.

The single greatest impediment to error prevention is that we punish people for making mistakes.
Dr Lucian Leape
In Culture of blame in National Health Service; Consequences and Solutions, S Radhakrishna explores how the health industry handles human errors. ‘The culture is to blame the individual for the error, rather than to try to understand the processes in the system that lead to the error.’[1] Her article discusses the medical and the legal paradigms, which Radhakrishna believes, are responsible for the culture of blame in healthcare.
‘The medical paradigm demands that the practitioner practises to perfection. It maintains that error is an ethical failure that constitutes an unprofessional act, which should be punished. Given that errors are not treated as human, errors may not be reported for fear of professional or legal reprisals. The legal paradigm’s approach to ensuring safe medical care is by rules of malpractice, which has been made more attractive with the no win-no fee banners.’[2] S Radhakrishna argues that medical and legal paradigms make individuals feel victimized, and because they are fearful of being blamed, they will not report errors. This inhibits frank discussions about errors and systems weakness.
Medical and legal paradigms put shackles on the health-care industry, whereas the systems approach is the way forward, that should take us out of the dreaded culture of blame.
S Radhakrishna
The Systems Paradigm

The systems paradigm is based on the principle that humans are fallible and that human errors are likely to occur in the best organizations. Errors are the result of a series of failures in the system and therefore are the consequences and not the causes. ‘The systems paradigm looks at the error as a cause of failures at several levels. It does not believe in ‘name and shame’ approach of the legal and medical paradigms. When an event occurs, it is not about who committed the error but, why the defences in the various layers failed.’[3] Radhakrishna argues that staff in such a set-up are more likely to report an error without fear, which will allow for real lessons to be learnt.
The NHS has an urgent need to implement the systems approach. A robust incident reporting system is the key to improving patient safety. A system that encourages data input, analysis and feedback without fear of punishment is likely to grow stronger.
My Case

My case is without doubt, a systemic failing. ‘The defences in the various levels’ have definitely failed. There is a complete systemic shut down of my case. Over 18 NHS bodies have now closed my case. I see a domino effect happening. One NHS body shuts my case down, and then the next one does the same, shortly afterwards. Because the systemic response is now so large-scale, no one individual will dare speak up on my behalf.
The situation with my GP is an example of how strong the systemic current is. When I first met him, 2 years ago, he was wonderful. He referred me to different departments for my facial pain, and said; ‘I know there is something seriously wrong with the left side of your face.’ He also expressed how terrible it is that ‘no one will take ownership of the problem.’ As NHS trusts rejected his referrals, or discharged me with no action taken, he and the practice have pulled down the shutters. The GP, who said two years ago, ‘there is seriously something wrong,’ writes two years later in my notes; scan abnormal, to be expected, no further action.
GP Shutdown

In the last year, this GP practice; 1) locked me out of my System One online account, while they amended a note on my medical records. They did this 18 months after they made the initial entry, which documents them not acting on an abnormal scan. This incident was after I told a clinician from Mental Health services, that I had seen this comment on my records. The clinician told the GP, with speed, that I had seen the comment. 2) There have also been three extremely serious incidents since then, which I have not yet blogged about. These further incidents involve the GP Practice deleting one entry and falsifying two medical entries. I will be writing about this at a later date, but this is the systemic behaviour with my case- to ignore and cover-up.
As Radhakrishna explains, individuals are afraid to speak up and report error because of the culture of blame and fear of reprisal. If someone within the system would vocalise what has gone wrong with my case, in an open and frank way, it could be put right. I would get the medical help that I need, and genuine lessons could be learnt. The systemic error is unlikely to flourish again.
The Code of Silence

In response to Radhakrishna’s article, a final year medical Student, Adam Shuttleworth, comments that ‘the reluctance to accept fallibility has led to the reporting of adverse events, which is labelled as “whistleblowing.” With this, there is an association with the placing of blame and “breaking silence.” He adds that a “code of silence” exists within medicine, in an effort to maintain a façade of perfection. Shuttleworth concludes that the ‘medical profession is yet to fully appreciate the safety in numbers.’ [4]
I see the ‘safety in numbers’ psychology with the clinicians and NHS bodies, involved my case, and it is chilling. They are complacent that it is safe to turn a blind eye to my medical problem. So many clinicians have done it too. Clinicians discharge me from clinics, when they know that there is a clinical issue. They also know that I cannot do anything to challenge them, so they are ‘safe.’
In Follow the Leader, I explain that it is like an endemic game of Chinese Whispers. When one NHS body is not transparent about clinical findings, or closes my case, it sends a signal to the next one. They then do the same. It is safer for these bodies to stay silent, rather than “blow a whistle.” I cannot find the words to convey how frightening it is to be on the receiving end of this behaviour. The unequal leverage of power is criminally unjust.
Respect and Curiosity

Rammya Mathew argues that clinicians have difficulty managing the conflict between avoiding humiliation for themselves, and honestly examining behaviour that does not meet expectations for which they might be responsible. ‘People do not need to be blamed in order to take responsibility and do better. We must make changes to improve care without needing to find someone to blame. This starts from a place of curiosity and respect.’[5] This is the crux of where the turning point is – replacing blame with curiosity and respect.
For healthcare, moving from a blame culture to one of rapid learning is critical to facilitate continuous improvement and innovation. A robust incident-reporting system, which seeks to identify root causes of incidents at a system level in order to prevent mistakes being repeated is key to enable this transition.[6]
Patient Safety
Patient Safety Learning uses the results of an NHS Staff Survey from 2020 on the safety culture, to explore the implications to patient safety within the persistent culture of blame in the NHS. The survey asked questions regarding action taken on reported errors and patient safety incidents. ‘More than 150,000 felt that they could not respond with confidence that their organisation takes action to ensure reported errors or incidents do not happen again.’[7] The survey also showed that the NHS does not act on concerns, that patients raise about patient safety.
Speaking Up

When an NHS worker speaks up, they are making a vital contribution to the quality and safety of patient care.
Sir Robert Francis, QC, 2015
The survey asked how safe staff feel about speaking up about errors, and patient safety incidents. Nearly a third of respondents said they do not feel safe to speak up. The survey also asked staff whether their organisation would treat staff involved in a patient safety incident fairly. 230,00 said this was not the case. In response to this, Henrietta Hughes, OBE states that; ‘there needs to be a more consistent approach from senior leadership throughout the health system to ensure that all workers are thanked, supported and listened to whenever they speak up.’[8]
Improving Safety Culture

To improve patient safety, it is important to move towards a just culture which considers wider systemic issues where things go wrong, enabling professionals to learn without fear of retribution, and to address incidents of unsafe care with empathy, respect and rigour.[9]
Patient Safety Learning, (PSL) argues that to ensure that patient safety incidents are reported and acted on, staff need to feel safe speaking up. They advocate for an “organisational culture that supports this.” They believe that the NHS should take the following actions, to improve the patient safety culture within the NHS;
- Ensure organisations measure and report on their progress in an open and transparent way.
- Enable organisations to share good practice for wide dissemination and implementation.
- Provide resources, guidance, support, and direction for organisations wanting to encourage staff speaking up.
- Proactively share examples where improvements have been made to speaking up cultures so lessons learnt can be shared widely and best practice implemented.
- Identify poorly performing organisations and intervene to make improvements.
- Report publicly on the progress and the impact that speaking up has had on patient safety and staff safety. [10]
Conclusion
As all of the summarised articles explain, we need to move away from a culture of blame. We need to move towards a culture where clinicians can report incidents without fear of reprisals. Incident reporting should not be used to apportion blame, but to drive systemic changes that improve patient care. Moving towards dealing with the systemic failing, instead of blaming individuals, is key to facilitate real learning in healthcare. Awareness of cases like mine have the potential to improve patient safety measures. They also highlight the urgent need for greater accountability and candour in healthcare. However, if we stay locked in a culture of blame and fear, and keep our heads buried in the sand, many more patients, like me, will continue to be harmed.
We need to get away from the culture of blame, and the fear that it generates, to one which celebrates openness and commitment to safety and improvement. The risks to patients’ lives and well-being will be reduced, and confidence in the NHS protected.[11]

Foot Notes
[1] Radhakrishna, S; Culture of Blame in The National Health Service; Consequences and Solutions, British Journal of Anaesthesia, Volume 115, Issue 5, ©Oxford University Press, November, 2015.
[2] Radhakrishna, S; Culture of Blame in The National Health Service; Consequences and Solutions, British Journal of Anaesthesia, Volume 115, Issue 5, ©Oxford University Press, November, 2015.
[3] Same source as footnotes 1&2.
[4] Shuttleworth, A J; Safety in Numbers- To Err is Human, September, 2015. (A Shuttleworth was a Final Year Medical Student at St George’s, University of London.)
[5] Mathew R; Lucy Letby and the Limits of a No Blame Culture, BMJ 2023; 382: p 1966
[6]Why a Culture of Rapid Learning in Healthcare is Vital www.improvewell.com
[7]Tackling the Blame Culture? NHS Staff Survey Results 2020 www.patientsafetylearning.org
[8] Hughes H, OBE; The National Guardian’s Response to the NHS Staff Survey Results, The National Guardian’s Office, March, 2021.
[9] Sir Norman Williams; Gross Negligence Manslaughter in Healthcare; The Report of a Rapid Policy Review, 3.4, P9, June, 2018.
[10] Tackling The Blame Culture? NHS Staff Survey Results 2020, www.patientsafetylearning.org
[11] Sir Robert Francis QC; Freedom to Speak Up; An Independent Review into Creating an Open and Honest Reporting Culture in the NHS, February, 2015.
Photo Credits; Sander Sammy, Designecologist, Tom Wilson, Jorge Flores, Brett Jordan, Mark Konig and Marco Bianchetti on Unsplash. Polina Kovalova on Pexels.

2024-05-04 10:08
On The No Win-No Fee Culture
Introduction
I’m an eighties child. Well, I was born in 1973. But, I came to life in Polka Dot leggings and badly crimped hair in the 1980’s. My memories of the adverts that aired on television in the early eighties, were commercials about the famine in Ethiopia. Towards the end of the decade, I mainly remember the adverts about the HIV/AIDS epidemic. There is a gap in my memory. I cannot remember the year that the Tsunami of ‘No Win-No Fee’ adverts hit the British shores. As a guestimate, I would say it was sometime in the early 1990’s.

‘No Win-No Fee’ culture refers to the free access that a claimant has to funding a medical negligence claim against a hospital or GP Practice for malpractice. If a solicitor takes on a case under a ‘No Win-No Fee’ agreement, the claimant will not be liable to pay any legal costs if they do not win the case. The ‘No Win-No Fee’ agreement has allowed many more people to make medical negligence claims.
The ‘No Win-No Fee’ culture is now a prevalent part of our society, and it has changed the landscape of doctoring and medicine, from one of care and love, to one of fear and defensiveness. The rampant suing culture has made doctors afraid and self-protective. This post discusses how the ‘No Win-No Fee’ culture has created a climate of fear and distrust and disabled the authenticity of the doctor-patient relationship.
Fear of litigation has resulted in significant harm to the quality of public services, the experiences of those who use them, and the role of professionals. The fear of litigation stifles innovation and leads to defensive practices.[1]
The Patient’s Perspective

When something goes wrong with patient care, patients want it to be put right. Lives are destroyed by medical accidents. Patients want their lives back. Three billion pounds would not buy me back the last eleven years. It would neither buy me back the woman who I was, and it would certainly not erase the traumatic memories that I have of these brutal consultations with surgeons.
However, if a clinician could diagnose and treat my facial pain, this would buy me my future. I would then be able to rebuild a normal life. The last thing that I would choose to do, is spend another decade wading through the judicial system. I reckon that 70% of the population would say the same. Yes, there are situations when it is right for a patient to bring a medical negligence claim against an NHS trust. But mostly, I think, patients want resolution. I certainly do.
After harm in healthcare, patients value patient safety efforts so that other patients do not need to endure the same suffering. Injured patients value disclosure and discussions that are compassionate, efficient, transparent, honest and include a genuine apology. [2]
An Incident

In 2019, I had a stern insight into the impact that the suing culture has on the doctor-patient relationship. I had an appointment to see a Head and Neck surgeon at an NHS Teaching Hospital. I had already been to this NHS Trust twice; once to the oculoplastic department re my periocular pain. They discharged me after one appointment with no diagnosis or treatment. I had also been to the Oral Maxillofacial Department, re the residual pain in my parotid gland. They too, discharged me after one consultation, with no offer of any help. This was my third visit to this NHS Trust.
I was waiting outside the consultant’s room. A nurse walked past me, carrying my notes, which she was delivering to the consultant. She dropped them on the floor, by accident. My file landed face up. I couldn’t believe my eyes. I saw a green medico-legal form, that the NHS trust had already filled in. They had begun a defence to a medical negligence claim, but I had not even been to see a solicitor. I had not filed a claim against them. This incident just demonstrates how fearful the medical landscape now is.

It was not a productive appointment. The surgeon was shifty and defensive, while I was reeling from the shock, from having seen the completed medico- legal form in my file. There was no space between us, for an honest or helpful conversation about my facial pain. We were both dancing around a puddle of fear.
Medical malpractice litigation stifles the patient voice and harms patient-provider relationship, by conceptualising patients as adversaries rather than partners. These issues hinder transparency and communication, and perpetuate distrust. Medical malpractice encourages defensive medicine.[3]
Non-Adversarial Resolution

The Standards Authority for Health and Social Care argues that a move to a non-adversarial clinical negligence system would ‘encourage a more open, constructive approach to clinical incidents, which would be beneficial to patient care and safety.’ (2.1) It states that ‘the fear of litigation is a key source of reticence among healthcare professionals in coming forward when avoidable harm has occurred.’ Their submission refers to a framework that was pioneered by The University of Michigan, that encourages early disclosure where things have gone wrong in healthcare. ‘The system has seen a drop in new lawsuits, and clinicians across U-M’s hospitals have felt freer to report situations that caused harm.’ (2.2) This has led to faster responses to investigate situations and reduced the chance of harm in the future.’[4]
Alternative Resolution Systems
Jennifer Schulz evaluates two other models of non-adversarial systems which resolve harm in healthcare; New Zealand’s Administrative Compensation Scheme, (ACC) and the USA’s Communication-and-Resolution Program, (CRP.) Shultz calls out for reform of England’s Medical Negligence system, and advocates for a no-fault compensation scheme, which values what patients want and need, after harm in healthcare. She argues that medical negligence litigation is misaligned with patients’ needs after harm. ‘Medical negligence litigation is an anathema to values in healthcare, particularly patient-centred care. It facilitates a “deny and defend” approach, whereas alternative approaches facilitate a “disclose and apologise approach.” The CRP and ACC no-fault schemes place the needs of the injured at the centre, which is consistent with patient-centred care, and values of honesty, disclosure, transparency and communication.’ [5]
NZ’s Accident Compensation Corporation (ACC)

- New Zealanders apply to the ACC scheme for rehabilitation and compensation. The compensation standard is ‘no-fault’ as opposed to negligence.
- The right to claim compensation is based on the injured person coming with the statutory conditions for cover, not on questions of liability. The first step for obtaining cover is that an injured person should get treatment from a healthcare provider.
- Remedies offered by the scheme include; treatment, rehabilitation, earnings compensation and a lump sum for permanent impairment, instead of solely compensation.
- The public can claim for ACC without the need for a lawyer. Patients are able to complete a simple document themselves.
- Fears about the ACC scheme are accountability. However, if an injured person applies to the ACC for compensation and rehabilitation, they can file a complaint with the NZ health and disability commissioner. The other criticism is that it removes deterrents to injury-producing conduct, which is disincentive to safety. Schultz explains that fault schemes do not have a deterrent impact. Medical malpractice has a deleterious impact. Health providers engage in defensive practises.[6]
Compassion

In the USA, Communication-and-Resolution Programs are the alternative to medical malpractice litigation, in which hospitals disclose medical injuries, explain what happened, apologise, and sometimes offer compensation. They only operate in a small number of healthcare organisations, but ‘they value patient-centred care, patient safety and patient’s needs.’ Shultz’s research found that patients value the compassionate and non-adversarial communication throughout the process, and the ability to heal broken trust between provider and patient. ‘Assuming patients and providers value, honesty, integrity, transparency, communication, trust, and meeting the needs of patients after medical injury, these approaches fulfil those values much better than medical malpractice litigation.’[7]
My Case

There was a lack of transparency about clinical findings early on. Ten-years on, when abnormality shows on tests, histology reports and scans, clinicians fear that if they acknowledge the findings and diagnose my facial pain, that they will make the preceding NHS trusts liable for litigation. That is why, I believe, abnormal results are not being acted on, and no-one will take responsibility for the problem. I also believe this is the unconscious incentive behind a lot of the gaslighting that I have experienced from medical consultants. All I want is for someone from the NHS to come out and say; ‘sorry, we have got this wrong, and we will put it right.’
Human Relationships

Relationships are messy. No human relationship can survive without one person at some point, needing to say sorry for bad behaviour. If neither side ever takes responsibility for the breakdown in the relationship, then the relationship sadly dies. Sorry is not a dirty word. It is a vital word, that salves the wounds of wrongdoing, and allows relationships to repair. Human’s make mistakes. ‘To err is human.’[8] We all get things wrong. It is an integral part of the human condition, and no-one is immune from fallibility, not even doctors.
If our human ability to make mistakes is stifled, we feel suffocated. The ‘No win-No Fee’ culture serves as a tight leash around doctors’ necks. It denies them any room for error and honest evaluation of their conduct. In denying clinicians this ability to self-evaluate, they cannot grow or improve.

Conclusion
Doctors are humans. They will, like all of us, make mistakes and get things wrong. This oppressive ‘No Win-No Fee’ culture disallows for human fallibility. It contributes hugely to the NHS Complaints Procedure being so futile. It is why, I think, clinical teams so routinely cover-up their failings. They fear that if they acknowledge wrong-doing, that they will make themselves liable to litigation.
Doctors need to be granted space to be honest when they get things wrong, without the fear that it will make them vulnerable to legal action. As the Professional Duty of Candour states; ‘Apologising to a patient does not mean that you are admitting legal liability for what has happened. The NHS Resolution advises that saying sorry is the right thing to do, and a fitness to practise panel may view an apology as evidence of insight.’ (15) [9]

The ‘No Win-No Fee’ Culture has had a crushing impact on clinicians’ ability to be authentic with patients. This tight leash around their necks must be loosened, to open up space for greater listening and authenticity within the doctor-patient relationship. Medicine is about healing, love and care, and these principles must be allowed to once again, govern the medical landscape.
England’s review of clinical negligence presents a timely opportunity to present an alternative resolution system to address patients’ needs after medical injury. In a climate where quality and safety, patient-centred care and compassion are heralded as important values in the health-sector, shifting away from medical malpractice litigation, that is misaligned with those values, is much needed.[10]
Foot Notes
[1] Clinical negligence: a culture of litigation? | Medical Negligence and Personal Injury Blog | Kingsley Napley | Independent Law Firm of the Year 2022
[2] Schulz Jennifer; Reforming Clinical Negligence in England: Lessons about Patients’ and Providers’ Values from Medical Injury Resolution in New Zealand and the United States of America © Royal College of Physicians, 2022.
[3] Schulz Jennifer; Reforming Clinical Negligence in England: Lessons about Patients’ and Providers’ Values from Medical Injury Resolution in New Zealand and the United States of America, © Royal College of Physicians, 2022.
[4] Written Evidence Submitted by The Professional Standards Authority (NLR0047) www.professionalstandards.org.uk. All quotations within this paragraph are quoted from this source.
[5] This is taken from the same source as footnote 2&3.
[6] This paragraph on NZ’s ACC Scheme is quoted directly from the same source as footnote 2,3 & 5
[7] Same source as footnote 2,3 & 5.
[8] Kohn L et al; To Err is Human; Building a Safer Health System-PubMed (nih.gov)
[9] The General Medical Council; The Professional Duty of Candour, www.gmc-uk.org
[10] Reforming clinical negligence in England: lessons about patients’ and providers’ values from medical injury resolution in New Zealand and the United States of America – PMC (nih.gov)
Photo Credits; World Sikh Org, Alex Green, Cottonbro, Tima Miroshnichenko, August de Richelieu & Mart Production on Pexels. Cytonn Photography, Dave Lowe, Hunters Race, Thomas Kinto & Brett Jordan on Unsplash.

2024-04-12 09:50
Is The PHSO Really Independent?
Introduction
The Parliamentary and Health Service Ombudsman, (PHSO) is a UK government agency, that was ‘set up by Parliament to provide an independent complaint handling service for complaints that have not been resolved by the NHS in England and UK government departments.’[1] The PHSO shares its findings from its casework ‘to help Parliament scrutinise public service providers.’ [2]The PHSO is not part of the government or the NHS in England. They are not a regulator. Their powers are set by The Health Service Commissioners Act, 1933.[3]

Our vision is a voice for improvement in public services through the provision of an independent, impartial and fair complaints handling service.
The Parliamentary and Health Service Ombudsman
This post discusses my experience of the PHSO. It also asks whether the PHSO is really independent, or whether it is a government agency that protects other government agencies. Is the PHSO really a government body that is committed to impartiality and fairness, or is it’s support biased towards the big organisations?
How It Works
If you are unhappy with the final response that you receive from the NHS body, you can take your complaint to the PHSO, who may investigate it. You need to bring your complaint to the PHSO within twelve months of receiving your final response from the NHS body. You also need to have exhausted the local complaints procedure first, and have received your final response from the NHS agency. The PHSO triage team will assess your complaint, and decide whether or not to open an investigation. If the PHSO decide to investigate it, they will allocate your complaint to a ‘case-worker.’ The wait time for allocation can take months.

Once allocated, a case worker will begin an investigation. They will ask the NHS agency to submit their version of events with supporting evidence. The case worker will get an ‘independent’ medical opinion from a clinician, who specialises in the field that is relevant to your medical case. The case worker sends you a provisional decision, at which stage, you can add your thoughts. The PHSO will then send both parties a final investigation report.
Recommendations

The PHSO either upholds, partially upholds, or does not uphold complaints. If the PHSO upholds or partially upholds your complaint, it can make recommendations to the NHS body to put things right. Recommendations can include; offering an apology, or devising a plan to show how they will prevent the same failing from happening again. If you are unhappy with the outcome from the PHSO, and you acquire new medical evidence, you can ask them to look at their decision again. You must do this within twelve months of receiving their final report.
After you receive their review outcome, if you think that the PHSO has acted unfairly or illegally, you can apply for a Judicial Review from the courts. You must make an application for Judicial Review within three months of receiving your decision from the PHSO. This all sounds hunky dory, right? The reality, however, is that once the administrative cogs are set in motion, it is not as peachy as it sounds.

My Complaint
In 2015, in the early stages of my facial pain, I took a multi-agency complaint to the PHSO about two NHS Trusts, who stopped my antibiotics when I still had an infection, and a GP Practice, who refused to then refer me to another specialist. I had to seek private care to get the blood tests and medication that I needed. This cost me £18,000 of borrowed money, and I did not get a satisfactory response to my complaint from the NHS agencies.

I provided the PHSO with the blood tests from the NHS trust, which showed evidence of infection, the Ophthalmologist’s clinic letters; one acknowledging an infection was present, and the other instructing the GP to stop my antibiotics. I submitted the blood tests from the private hospital, showing that I still had an infection, and a statement from my MP, who I went to see at Parliament when this happened. He verified that he spoke to my then GP, who told him they would not refer me to another Ophthalmologist, unless I found a specialist, and if they agreed with their diagnosis. I requested that the NHS Trusts reimburse me my costs for blood tests and medication.
My Experience

I went into the PHSO process naively. Not dissimilar to how a child envisions Jesus Christ, as a bearded man in the sky, I imagined the Ombudsman to be a person sitting in the middle, holding the scales of justice, and giving both sides a decent hearing. That couldn’t be further from the reality. The Health Ombudsman, who in 2015, was Dame Julie Mellor, does not see the complaints. The complaints are dealt with by low-skilled case workers, who act more as secretaries. It is their managers and the medical teams behind the scenes, who make the decision.
It is not a ‘fair’ or equal set up from the start. I sought help from the Citizens Advice Bureau, who assisted me with my PHSO complaint form. However, even with advocacy support, I could not match up to the defence unions and powerful legal teams that the NHS bodies had to assist them. I was knocked out before the match had started.
‘Reasonable?’

‘Reasonable’ is a vague term, with far-reaching boundaries, when used in administrative processes. The bench mark that the PHSO uses to decide if there has been any malpractice or maladministration, is whether the NHS body acted ‘reasonably’ or not. An ophthalmologist, who admits a patient for intravenous antibiotics because there is clinical evidence of infection, and then discharges them, and instructs the GP to stop all her medication, without doing a blood test, to see if her infection markers have normalised, is not reasonable. For the GP to refuse further referrals, is unfair, and it left me in an unfathomable predicament.

I felt both aghast and outraged, (as was my advocate) when the PHSO sent me their provisional report. They had overlooked all of my evidence, and had defended the actions of the NHS Trusts and GP, as being ‘reasonable.’ Their report had gaping holes in it, and swerved the facts. Their ‘medical advisor,’ who had never examined me, said that my left ptosis, which was diagnosed by a Professor of Ophthalmology, after the first ophthalmologist had stopped my treatment, was not true. The PHSO also said that I ‘chose’ to seek private care. The NHS Trusts and GP stopped my medication and blood tests, and I became very ill. They also closed the doorway to any more referrals. I had no choice. My MP verified this in a statement, which the PHSO also disregarded.
PHSO Review
![]()
I asked the PHSO to look at their decision again, on the grounds that they overlooked my original evidence. I also submitted new medical evidence, along with a revised statement from my MP. It took them an unreasonable eleven months to complete their review. Their procedure was more dishonest than the first round. They discounted and undermined my new evidence, and neglected to honour my MP’s statement. The PHSO still concluded that I chose to spend £18,000 to get medication privately. They also said I could have moved GP’s, when I supplied them with data, that no other GP would accept me, as I was outside of their catchment area.
For a body that prides itself on values of ‘independence, ‘fairness,’ ‘excellence,’ and ‘transparency,’ their service did not reflect any of these principles. Their conduct represented dishonesty, unfairness, bias and a poor-quality service, with unreasonable wait times.
Judicial Review

Public bodies have to obey the law in how they take decisions and act. [4]
I quickly found a public law solicitor, who took on my case for Judicial Review. This was to challenge the fairness of the PHSO’s approach to handling my complaint. Judicial Review is ‘a court proceeding in which a judge reviews the lawfulness of a decision made by a public body. It challenges the way in which a decision was made, rather than the conclusion reached.’ [5]The courts can issue a quashing order, which overturns the decision, or a mandatory order, where the court directs the body to take a new decision. They can also award damages, if your human rights have been breached.
My Grounds For Judicial Review

The details of the matter being challenged were, The PHSO’s:
- Failure to appropriately exercise its discretion in relation to my case;
- Failure to take into account relevant considerations and/or taking into account irrelevant considerations;
- Failure to undertake sufficient enquiries into why I was unable to seek the assistance of another NHS GP in January, 2014;
- Failure to ask the questions necessary and undertake a sufficient enquiry to discharge its decision-making process;
- Decision is unreasonable/irrational in the Wednesbury sense. The grounds for this are:
- The decision was unreasonable or irrational in the Wednesbury sense;
- Material error of fact;
- Failure to undertake a sufficient inquiry by asking the right questions or taking reasonable steps to acquaint themselves with relevant information;
- Taking into account irrelevant considerations or ignored relevant considerations;
- The discretion of the Respondent in the application of its policy was fettered.
The legal aid Agency awarded me legal aid to cover the first stages of Judicial Review; the Pre-Action Protocol and request for permission. We served notice on the PHSO and submitted a permission request for Judicial Review from the courts. The PHSO submitted a lengthy, (and late) defence. I received an offer from the court to attend an oral hearing, to request permission from the Judge. However, the process had exhausted me, so I declined the offer of an oral hearing. I dropped the case. This is how the system works. It asks people to jump through extensive loopholes, which grind down the individual’s resolve. These administrative processes do not support the individual having a voice.

Rob Behrens
I have been heartened by the reports from the current Health Ombudsman, Rob Behrens, who has come down hard, on the lies and cover-up culture within the NHS. I wondered whether he had transformed the culture within the PHSO; that they now acted more in accordance with their values and held NHS bodies more to account? However, according to people who I have spoken to, the service that the PHSO provide is even worse. They open even fewer investigations than they did in 2015. If this is correct, then the PHSO is guilty of the very thing that Rob Behrens is so scathing of; covering up failings, and not being accountable for mistakes.
Conclusion

My experience of the PHSO was crushing. They overlooked factual evidence, and did not look at my complaint honestly or fairly. They were heavily biased towards the NHS Trusts and GP Practice. Many others have had similar experiences to me. The PHSO, in my experience, is not an independent or impartial body. It is a body that is predisposed towards the state funded organisations. There is little listening or support for the little man/woman, who has suffered an injustice within the UK healthcare system. If there was, I would not be in the predicament that I am in now. The question that my and many other’s experience raises, is how can the PHSO really improve public services, if the PHSO does not look into complaints with real impartiality and fairness?
Foot Notes
[1] www.ombudsman.org.uk/who we are
[2] https://www.ombudsman.org.uk/about-us/who-we-are
[3] This comes from the same source as foot note 1 & 2.
[4] The Public Law Project; An Introduction to Judicial Review.
[5] https://www.judiciary.uk/how-the-law-works/judicial-review/
Advocacy Resources
These are UK wide agencies, who can provide advocacy support with the PHSO complaints process.
NHS Complaints Advocacy | POhWER
Find your local Healthwatch | Healthwatch
York Advocacy Hub – NHS Advocacy
VoiceAbility | NHS complaints advocacy
Independent Health Complaints Advocacy (IHCA) – Advocacy for Bromley
Judicial Review Resources
These are useful resources for anyone wanting to challenge the fairness and legality of a PHSO decision.
Apply for a judicial review of a decision: Form N461 – GOV.UK (www.gov.uk)
Find a Solicitor – The Law Society
Judicial Review and other Public Law Challenges | Bindmans
Check if you can get legal aid – GOV.UK (www.gov.uk)

Photo Credits: Tingey Law Firm, Mufid Majnun, Gr Stocks, Yaopey Yong, Lucas Santos, Brut Carniollus, Gayatri Malhotra, D Koi and Nsey Benajah on Unsplash. Anete Lusina, Katrin Bolovtsova and Sora Shimazaki and Brett Jordan on Pexels.

2024-03-28 07:14
On The NHS Complaints Procedure
Summary
This post debates the NHS complaints procedure, within the context of The Professional Duty of Candour. I discuss my experiences of the NHS complaints procedure; how clinical teams rarely self-evaluate or reflect on their conduct, during investigations. They seldom take any responsibility when things go wrong with a patient’s care. This makes the NHS complaints process futile for patients, and devoid of any transparency. This post asks how the NHS complaints procedure can work better for patients who are seeking redress to genuine grievances?

The NHS Constitution

‘Everybody has the right to make a complaint about any aspect of NHS care, treatment or service, and this is written into the NHS Constitution on GOV.UK.’[1] The NHS pledges to:
- ensure that when mistakes happen or if you are harmed while receiving health care you receive an appropriate explanation and apology, delivered with sensitivity and recognition of the trauma you have experienced, and know that lessons will be learned to help avoid a similar incident occurring again
- ensure that the organisation learns lessons from complaints and uses these to improve NHS services[2]
The NHS Complaints Procedure
Any patient can send a complaint to an NHS trust, by email or post. Once the NHS trust receives the complaint, a member from the complaints team will send an acknowledgement to the patient, within 2-3 days. This will confirm that the patient’s complaint has been received, and sent to the clinical ‘team manager.’ This is not a clinician. The complaints team will forward the complaint onto the administrative manager of the clinical team. The manager will then contact the patient, to check that they have understood the points that the patient has raised in the complaint.
The team manager will ‘investigate’ the complaint, by speaking to the medical professionals involved, and looking at the patient records. They will send the patient a formal response within 28 days, which the Chief Executive, (CEO) of the NHS trust signs. The report provides details of the Parliamentary Health Service Ombudsman, (PHSO) who the patient can refer to, if they are unhappy with the response from the NHS trust.
The Duty of Candour

‘The intention of the duty of candour legislation is to ensure that providers are open and transparent with people who use services. It sets out some specific requirements providers must follow when things go wrong, with care and treatment, including providing reasonable support, providing truthful information and an apology when things go wrong.’ It states that, ‘Registered persons must act in an open and transparent way with relevant persons in relation to care and treatment provided to service users in carrying on a regulated activity.’[3]
Good Medical Practice

Good Medical Practice states that doctors ‘must’;
45 be open and honest with patients if things go wrong. If a patient under your care has suffered harm or distress, you must follow our guidance on Openness and Honesty when things go Wrong; the Professional Duty of Candour, and you should:
a put matters right, if possible
b apologise (apologising does not, of itself, mean that you are admitting legal liability for what’s happened)
c explain fully and promptly what has happened and the likely short-term and long-term effects
d report the incident in line with your organisation’s policy so it can be investigated as appropriate – and lessons can be learnt and patients protected from harm in the future.
46 You must respond promptly, fully and honestly to complaints. [4]
Every health and care professional must be open and honest with patients and people in their care, when something goes wrong with their treatment or care, and causes harm or distress. General Medical Council
The Professional Duty of Candour

The General Medical Councils’ Professional Duty of Candour makes clear that; ‘all healthcare professionals have a duty of candour – a professional responsibility to be honest with patients when things go wrong.’ Healthcare professionals ‘must’
- Tell the person when something has gone wrong
- Apologise to the person
- Offer an appropriate remedy to put things right
- Explain fully the long-term effects of what has happened.[5]
It states that a professional must apologise to the patient; ‘when something goes wrong with their care, and they suffer harm or distress as a result.’ (9) It instructs that doctors ‘should share all you know and believe to be true about what went wrong, and why. You should explain if anything is still uncertain and you must respond honestly to questions. You should apologise to the patient.’ (12)
Saying Sorry

The Professional Duty of Candour sets out that patients expect to be told three things as part of an apology;
- What happened
- What can be done to deal with any harm caused
- What will be done to prevent someone else being harmed. (14)
It makes clear that ‘apologising to a patient does not mean you are admitting legal liability for what has happened, and that the NHS Resolution advises saying sorry is the right thing to do.’ (15) The Professional Duty of Candour advises against a ‘formulaic approach to apologising, since an apology has value only if it is genuine,’ (17.) It states that when apologising to a patient, you should consider that; ‘patients find it more meaningful if you offer a personalised apology, rather than a general expression of regret about the incident on the organisations behalf.’ (17.d)[6]
The Professional Duty of Candour also encourages a learning culture. ‘When something goes wrong with patient care, it is crucial that it is reported at an early stage, so that lessons can be learnt quickly and patients can be protected from harm in the future.’ (23)[7]
My Experience

Having read the Professional Duty of Candour, I feel short-changed. I have complained to five out of the fifteen NHS trusts that I have been to for my facial pain. My complaints have ranged from consultants stopping my antibiotics when I still had an infection, forcing me to pay for private treatment, to clinicians prematurely discharging me, clinicians not following through on promised actions, and consultants being rude and insulting. I have not once received an apology or any honest explanation of what went wrong. I have not had any of my grievances put right.
What I have received, is a defensive explanation of their view of the situation. This leaves me feeling unheard and more hurt as a result. The NHS trusts swerve key points that I have raised. They use blanket statements like; ‘lessons have been learnt,’ but the NHS trusts never specify what lessons they have learnt. This makes wording of this nature, nothing more than a platitude. All responses that I have received have lacked any self-evaluation from the clinicians involved, or willingness to take any responsibility for the failings that have caused me harm. This has left me to carry the unresolved grievance, alone.
The Worst Response

The shoddiest response that I received, was from an NHS Trust in Scotland. The surgeon, who I saw, had promised to do two scans and see me for a follow-up, but I never heard from him again. I complained to the NHS trust that the surgeon did not give me a follow-up consultation and closed my case, with no explanation. He had referred me to Pain Management. They had refused to see me, because I was not ‘suitable’ for their service. I received no answers from the NHS trust about the surgeon’s decisions. The NHS trust just advised in their response, that I ‘go to pain management,’ when they knew full well that Pain Management had refused to see me. They led me down a dead end, which they knew was a dead end. This behaviour is quite the opposite to being ‘open’ and ‘honest.’
The Ombudsman’s report found the physical harm patients suffer following mistakes is often “made worse” by “inadequate, defensive and insensitive responses” from NHS Trusts. [8]
What Patients Want

Patients want hearing and validating. They want answers about what has gone wrong. They want an apology, and they want the issue putting right. All I have wanted is an honest explanation about why has gone wrong with my care, and for the NHS trusts to remedy it. I have not received this, so I have stopped raising complaints. There is no point. I just come up against a brick wall, every time that I try to get answers.

Conclusion
The responses to my complaints have not complied with The Professional Duty of Candour. Clinician’s failings have caused me genuine harm, which they have not acknowledged, or put right. This begs the question – what is the use of having an NHS complaints procedure, if ‘investigators’ just defend clinician’s mistakes? How can medical teams ‘learn lessons,’ from failings in care, if they are not honest about their mistakes, and do not evaluate themselves candidly?

To ensure that medical teams adhere to The Professional Duty of Candour, professionals need to listen to patients more openly, and learn to say sorry. Apologising is not an admission of legal liability. It is an avenue for redressing grievances, improving services, and preventing further harm. Abdicating from taking responsibility for their failings does not serve the medical professionals either. Rigorous self-scrutiny should be at the top of the agenda for self-regulating doctors. Without this, clinicians cannot develop professionally, and will repeat the same mistakes, causing more harm to future patients.
The Ombudsman’s report pointed to “confirmed failures to accept mistakes” and the failure of some NHS trusts to “take accountability” for turning lessons into actions.
Jane Kirby, The Standard.
Foot Notes
[1] https://www.nhs.uk/contact-us/how-to-complain-to-the-nhs/
[2] Department of Health and Social Care, GOV.UK; Guidance NHS Constitution for England, March, 2012
[3] Guidance Duty of Candour GOV.UK October, 2020
[4]General Medical Council; Good Medical Practice, 2024. © 2023 General Medical Council.
[5] General Medical Council; Openness and Honesty when Things go Wrong: The Professional Duty of Candour, ©2015 General Medical Council. Note; This is joint guidance with the Nursing and Midwifery Council, (NMC.)
[6] General Medical Council; Openness and Honesty when Things go Wrong: The Professional Duty of Candour, ©2015 General Medical Council. Note; This is joint guidance with the Nursing and Midwifery Council (NMC.)
[7] Extract from same source as foot note 5 & 6.
[8] Kirby Jane; Ombudsman Finds “Culture of Cover-Up” in NHS When Patients Are Harmed, The Independent, June, 2023.
Photo Credits; Matthias Zomer, Shvets Production, Alex Green, Trung Nguyen, Ann H and Antoni Shkraba on Pexels. Doctor, Tim Mossholder, Randy Laybourne, Nicolas J Leclercq and Nick Fewings on Unsplash.

2024-03-15 12:07
This Is A Cover-Up
Introduction
The cover-up culture is currently rife. Stories of institutions covering up abuse, are hitting the headlines at a pace. As I watch stories like The Vagina Mesh scandal, The Lucy Letby case and The Post Office scandal come to light, I can relate. My story, whilst not yet exposed, is a cover-up. There have been many incidents, where clinicians have not been honest about clinical findings, and have covered up evidence. Institutions now cover-up for one another by default.

Aside from the burning pain of injustice, it is heartrending feeling silenced by an inhumane system, that protects its own. My intelligence has been insulted, so it is vital to me, that the clinicians who have been involved, know that I have clocked every occasion, when a clinical finding has been covered up, medical records have been amended, and the truth has been hidden.
I am writing about this sensitive subject, because I want to see change. One woman’s story is potentially every woman’s story, and I do not want to see another person go through what I have. I want to see more transparency with clinicians, and more accountability for how doctors behave. Personally, I am living with a level of fury and despair, that I cannot carry alone anymore. I have to speak. Everything that I chronicle in this post is true and accurate. If there are consequences for me speaking out about this, I will happily accept them. I will not remain silent about clinicians who are neglecting their duty of care, and in some cases, breaking the law. A story like mine has the potential to inform change, and it is vital that voices like mine are heard.
There is a culture of cover-up in the NHS. There is no point pretending that everybody is nice and does the right thing.
Rob Behrens, Health Ombudsman
Incident 1

A private rheumatologist referred me to an Oral Maxillofacial surgeon, re the pain in my left parotid gland. I saw this surgeon at a Salivary Gland department, at a London NHS Hospital in February, 2016. The first sialo gram that he did showed obstruction in my parotid gland, which he washed away. When the surgeon wrote back to the referring rheumatologist, he did not mention in his clinic letter, that they had found obstruction in my gland.
The rheumatologist referred me back to the surgeon in June, 2016. A different consultant did an ultrasound, which showed a thickening of saliva, known as ‘mucous plugging.’ The consultant referred me for a Sialendoscopy. In December, 2016, I saw a registrar at the unit, who did the sialendoscopy. When she entered the endoscope into my papilla, we both saw on the screen, at the top of my parotid duct, big clumps of what looked like white clouds. ‘It’s bad in there,’ she said. ‘I am going to refer you for wash-outs, every 6 weeks.’ She handed me a green form, which I gave to the receptionist as I left the building.
A Dental Radiologist

I received an appointment to see the Head of Dental Radiology one month later. She works closely with the surgeon, who initially referred me to the unit. His initial referral letter had said; Please do these investigations, to prove that there is nothing wrong. This dental radiologist did a second sialendoscopy, which was incredibly healing. On leaving the procedure room, I asked her when I would hear from the consultant. ‘I haven’t written my report yet,’ she said.
In February, 2017, I saw the female consultant. ‘I’m discharging you,’ she said. ‘Everything is normal.’
‘That doesn’t make sense,’ I replied. ‘The registrar referred me for ongoing wash outs only 6 weeks ago?’
‘The dental radiologist has said that everything is normal.’
She appeared. There was a kafuffle between us. ‘Everything is fine,’ the dental radiologist said.
‘How can so much of changed, from when I saw the registrar 6 weeks ago?’
‘Maybe that was a mistake,’ she replied.
They discharged me. Case closed. I wrote to the NHS Trust and complained that the salivary gland unit had prematurely discharged me, only 6 weeks after the registrar had assessed me as needing regular wash outs of my gland. They sent me an appointment to return to see the lead dental radiologist.
Trip!

When I returned to see the Dental Radiologist at the salivary gland unit, she tripped. There were four registrars in the room, who were preparing for the procedure, while the dental radiologist was doing an ultrasound of my parotid gland.
‘You haven’t frozen the image!’ One of the registrars whispered, pointing to the screen.
‘Oh yes, silly me,’ the dental radiologist replied, and clicked on the mouse.
I jumped out of the chair. ‘Have you not been freezing my ultrasound images?’ I asked. The registrars looked down. ‘I can’t go through with this,’ I said. ‘You are not an honest clinician.’
‘But we need to do this procedure, Felicia. Your gland is not working as it should.’ That’s where she tripped.
‘You’ve just admitted that my gland is not working! I was discharged from here six weeks ago, because you told the consultant that “everything was normal.” You are not being honest about these findings,’ I said.
‘She’s just having a wobble,’ the dental radiologist said to the registrars.
‘No, this isn’t a wobble,’ I replied. ‘I cannot trust you.’ I walked out.
The dental radiologist had not told the truth. This was proven in the histology report from my superficial parotidectomy 1-yr later, which showed dense secretions in the ducts and numerous calcifications. Each time I see a new clinician, they phone the dental radiologist for her opinion. She tells them that everything was normal. They believe her, and the fib is perpetuated.
I see evidence where patients have been lied to, and there are a whole series of incidents where people do not know what went on and hospitals are reluctant to disclose this. You can call it whatever you like but it is a cover-up.
Rob Behrens, Health Ombudsman
Incident 2
In May, 2019, I saw a Head and Neck surgeon at another NHS Trust in London. He is a close colleague of the surgeon mentioned above. In; On Medical Gaslighting #1, I explain that it looks possible, that this NHS Trust have deleted some images from an MRI Neck scan. After 4 scans, I saw on the surgeon’s screen, a radiology image with white blobs on the left side of my face. I asked him if they were calcifications. He said ‘no,’ and turned his computer off. I asked to see the image again, but he refused.
I requested the radiology images from the NHS Trust. When I received the disk, there was a missing file icon next to the MRI Neck Scan. When I clicked on that scan, a sign appeared which said; error decoding images. I queried this with the NHS Trust, and they told me that they had merged those images with another scan. That may be true, but I cannot find the images on the disk that I have, that I saw on the surgeon’s screen in 2019. I think that it is possible, that a series of images may have been deleted, as part of this cover-up.

Image, showing missing file icon, next to MRI Neck scan with contrast.

Image shows what I see when I click on the MRI Neck Scan.
Incident 3
I have a query re the transparency of the radiologist, who reported on my CT Neck radiology images in July, 2020 at an NHS trust in Scotland. He reported everything as ‘normal,’ but there is a stark asymmetry between the two sides of my face, that still needs explaining.

Radiology Image from CT Neck scan, July, 2020

Radiology image from CT Neck scan, 2020.
In; On Mental Health Discrimination #1, I chronicle how a Head and Neck surgeon wrote a discriminatory comment about me on the scan request form, which he sent to this radiologist. I believe that the surgeon’s comment may have caused this radiologist to not report truthfully about these radiology images.
Incident 4
I saw an ENT consultant at an NHS Trust in England in July, 2022. He ordered an MRI Neck scan, which showed abnormality in my left buccal fat pad.


I saw an Oral Maxillofacial surgeon, who had the radiology report, which confirmed the abnormality, in front of him. During a horrendous consultation, the surgeon proceeded to change my radiology images on his screen, saying that the images are ‘squint’ and ‘off axis.’ I showed him CT radiology images that I had on my I-pad, and he told me that the quality of my I-pad was s**t. The surgeon gave me no explanation about my abnormal MRI scan. He took no action.

Incident 5

At this time; July, 2022, I logged into my TPP System One account and saw that my GP had written in my medical records; Scan abnormal. To be expected. No further action. This was shocking. Whilst I have sympathy for how consultants have ghosted my GP’s, a GP still has the power to ask questions and advocate for the patient. This GP has done neither. They have pulled down the shutters, and colluded with the cover-up.
A serious incident occurred with my GP re this comment. On 8th December, 2023, I attended an appointment with the Mental Health Team to request medication to aid my sleep. I told a clinician from the team that I had seen my GP’s comment on my medical records. When I got home from the appointment, I logged into my TPP System One account, but my username and password, that I had used for 2 years, did not work. I tried it many times, but I was locked out.
On 12th December, I phoned the GP practice. I told them that they had blocked me from entering my account. They provided me with a new username and password. To my horror, when I entered my online account, I saw that between 8-12th December, 2023, my GP had amended that comment. They had added to the entry; Review not applicable.

GP entry re scan in July, 2022. Review Not Applicable, is the amendment that the GP made between 8/12/23-12/12/23.
Good Medical Practice
Good Medical Practice states that a doctor ‘must’ make sure that formal records of your work, (including patients records) are clear, accurate, contemporaneous and legible.’ (69) [1]The footnotes explain that contemporaneous means making records at the same time as the event you are recording, or as soon as possible after. ‘You must,’ is used for a legal or ethical duty you are expected to meet.’ [2]My GP making an amendment to my record, 17 months after the event, is not contemporaneous. The GP has not adhered to their legal duty.
Amending Records

The Medical and Dental Defence Union (MDDUS) state that late additions to notes ‘should be added, with a clear note alongside explaining when the note was made, and the reason for the delay.’ MDDUS states that ‘clinicians must have a legitimate reason to alter a patient’s record. Any changes must be clearly marked, showing the name of the person making the change and the date the change was made.’[3]
When making changes to electronic records, the principle of transparency is paramount. Any alterations found to have been made without an accompanying explanatory note, such as the insertion of new notes, will be viewed seriously by the regulators and could lead to accusations of dishonesty.
Medical Dental Defence Union, Scotland
I felt threatened by this incident, particularly by how quickly the Mental Health team blew the whistle to the GP. The GP has not added any explanatory note, explaining why this amendment was made, when, or by whom, anywhere on my records. The black line in the image above is the doctors name being marked out. I can see no ‘legal basis,’ or ‘justifiable cause’ for the GP to have made this amendment, 17 months after the event, apart from the GP practice covering their backs. This incident was particularly concerning, in light of the fact that there was a serious incident at my GP Practice, which hit the headlines, only four months before they amended my records.
Never alter patient records without a legal basis or other justifiable cause.
Medical Dental Defence Union, Scotland
It’s Endemic

This cover-up is bigger than the individual clinicians involved. It is now endemic, which is why I have 1) stopped going to consultations, and 2) not moved to my eighth GP Practice. It keeps happening, and it won’t change until there is a paradigm shift. Clinicians keep up the falsehood, because if one of them was to admit there is actually a clinical problem, the House of Cards would fall.
Reflection

It is menacing how complacent these institutions are with behaving in this dishonest way. There’s a safety in numbers psychology; clinicians cover-up, which gives colleagues the license to do the same. My GP clearly thinks nothing of amending my records. What is so sinister, is that when I turned to the Mental Health Team for support, they told me to ‘reframe’ the situation, that ‘I don’t like what I hear.’ To put the responsibility of 11-years of systemic duplicity onto me, when one of their clinician’s has recently been complicit in the cover-up, is scandalous.
Every time an NHS scandal hits the front pages, leaders promise never again. But the NHS seems unable to learn from its mistakes and we see the same repeated failings time and time again. Health Ombudsman
Rob Behrens
Rob Behrens, the Health Ombudsman published a report into the cover-up culture in June 2023. He points to “the gaping hole” between policies aimed at improving patient safety and real-life experience on the ground, with hospitals “routinely” failing to accept their errors. His office highlighted continued failures to accept mistakes. He states the main causes of harm are; failure of staff to make the right diagnosis, delays in giving treatment, and a failure to listen to patients. Further harm is caused to patients when NHS trusts carry out poor quality investigations, fail to learn, and offer inadequate apologies.’[4]
Philip Schofield Scandal

I want to draw on the candid interview that Phillip Schofield gave to the BBC in June, 2023, after it emerged that he had been having an affair with a younger runner at This Morning. Amol Rajan asked Phillip ‘Why now? Why has this all come out now? What was the catalyst? Phillip answered; ‘The lie just got too big. It started as denial. It turned into a lie. The lie grew legs, and then it just got way too big.’
My medical story started with denial. The dental radiologist then didn’t tell the truth. Other clinicians believed her and felt that they had to be loyal to the deceit. The lie built and has grown legs. Now it is so big, that clinicians are backtracking on clinical findings and amending records. Gaslighting has become the dominant tactic to keep me silenced, which has become too threatening. That is why I have walked away.

Conclusion
These incidents have traumatised me, particularly the recent incident with my GP, locking me out of my account and amending my records, without being transparent about why. I have not slept properly since and my mood has become dangerously low. This has to stop. I need to know the truth; what is causing my facial pain, and what can be done about it. These medical professionals need to start being honest. It is not serving them to be getting away with deviating from GMC guidance like this. This is a cover-up. It is time for some long-awaited truth, accountability and liberation for everyone involved.
Cover-ups of mistakes must be challenged and accountability has to be at all levels. We need to see significant improvements in culture and leadership.
Rob Behrens, Health Ombudsman

Foot Notes
[1] The General Medical Council; Recording Your Work Clearly and Accurately; Good Medical Practice. Published August, 2023.
[2] The General Medical Council; Good Medical Practice. Published August, 2023.
[3] Altering clinical Records-Do’s and don’ts; MDDUS, mddus.com
[4] Kirby J; Ombudsman Finds ‘Culture of Cover-Ups’ in NHS When Patients Are Harmed, The Independent, June, 2023.
Recommended Articles
https://www.ombudsman.org.uk/news-and-blog/news/nhs-must-make-patient-safety-more-just-promise
Photo Credits; Tina Miroshnichenko, Daniel Frank, Markus Winkler and Andrea Piacquadio on Pexels. Ocean Bigshott, Daniel Monteiro, Mark Stuckey, Priscilla Du Preez, Jacki Drexler, and Sigmund on Unsplash.

2024-03-01 09:14
My 11-Year Diagnostic Delay
What Is Diagnostic Delay?
A diagnostic delay ‘occurs when a patient seeks medical treatment for symptoms, and yet the condition causing those symptoms go undiagnosed for an unreasonable amount of time. Often this may result in the condition worsening into a serious illness or disease. A delayed diagnosis might be the result of certain symptoms being overlooked or dismissed by the physician, or when the physician fails to order follow-up testing to fully evaluate the patient.’[1] This post discusses how my 11-year diagnostic delay for my facial pain has come about from clinicians overlooking clinical evidence and choosing not to act.

Overlooked Evidence
A painful aspect of my quest to find a resolution to my facial pain has been clinicians overlooking clinical evidence that has detected abnormality. There are some conditions that doctors struggle to diagnose due to a lack of unequivocal evidence. Endometriosis and fibromyalgia are two examples of such diseases. In my case, however, there has been a lot of clinical evidence that has pointed to an irrefutable clinical problem. All of the clinical evidence and pathology found points to infection as the likely cause of my facial pain. However, medical professionals have disregarded this evidence. Four infectious disease consultants found clinical signs of infection in blood tests but have taken no action. Dental radiologists detected salivary glandular malfunction and parenchymal damage but have not taken action beyond temporary glandular wash-outs. One NHS Trust and my GP have recently turned a blind eye to an abnormal MRI neck scan.

My medical condition is not ‘atypical facial pain’ or ‘chronic pain.’ Clinicians have detected lots of pathology. There is something that is causing my facial pain. However, if clinicians keep ignoring the clinical evidence, they will never identify an aetiology. Aside from infection or inflammation, what else could cause the following:
- Raised neutrophils, white blood count, ESR and haemoglobin count
- The levitator on my left eyelid to collapse
- Glandular malfunction and parenchymal damage
- Reactive lymph nodes
- Enlarged masseter muscle
- Unexplained abnormality in my buccal fat pad
- I respond to antibiotics, and no other medication?
Referral Tennis

My diagnostic delay has played out via a long game of referral tennis. Clinicians have passed me onto their colleagues instead of dealing with the problem themselves. It’s a Merry Go-round. My GP will refer me to a specialist in secondary care. The consultant sees me. He/she does a scan. He/she will then refer me to their colleague at another hospital. That hospital normally sends it back. They may give me one appointment, but then they close my case. The process starts again. The time scales are ridiculous. I can wait up to four months from the point that the GP refers me to a consultant to when I see a consultant. The time scale is the same when a consultant refers me onto his colleague. Eight months can pass. In those eight months, I am living with worsening pain.
It seems that clinicians think that referring me on to colleagues amounts to ‘action,’ when it actually amounts to delay-in-action. I cite an example; in July 2022, an Ear Nose and Throat consultant did an MRI scan. He wrote to me to tell me that they found an abnormality in my buccal fat pad and that he had sent my case up to a different department at another hospital. That hospital sent it back, telling the referring consultant that the ‘ball is in his court.’ The ball was batted off-pitch. I am not a tennis ball. I am human being. This is a human life not a game.

Apathy
The tone of the referral letters is apathetic. ‘Please will you review this lady, who has a history of unexplained facial pain.’ The next consultant greets me with a furrowed brow. I spend an hour explaining what my symptoms are. He takes notes and does what the preceding consultant did. He refers me on to one of his colleagues.
Diagnostic errors or delays (DEODs) remain an understudied threat to patient safety, occurring in up to 20% of patient-clinician encounters. A DEOD has been defined by the National Academy of Medicine (NAM) as a failure to establish an accurate explanation of the patient’s health problem or to communicate that explanation to the patient and within the health record.7 Singh classified DEOD, more recently as “missed opportunities” to make a diagnosis.8’[2]
Diagnostic Delays in Infectious Diseases

M. Suneja conducted a survey to examine diagnostic delays in six infectious diseases. ‘The objective was to understand the frequency of diagnostic delays commonly seen by infectious disease consultants and to examine contributing factors for these delays.’ [3] The results showed that the main causes of delay when diagnosing an infectious disease were:
- Diagnosis not being considered initially
- The appropriate test not being ordered
- Unusual clinical presentation
- Not consulting an Infectious Disease Consultant early enough.
A Missed Opportunity

I saw the first infectious disease specialist 3 years into my illness. It was in 2016. I saw him at a large NHS teaching hospital in London. He did some blood tests. They showed that my neutrophil count was high. I was also under the care of the ophthalmology team and oral maxillofacial surgeon at the same NHS trust. Ophthalmology diagnosed my left ptosis and told me the levitator had collapsed. The oral maxillofacial surgery team found that my left parotid gland was not functioning properly. They treated my glandular malfunction with regular wash-outs.
This was a perfect opportunity for all three departments to collaborate, examine the collective evidence, and act, but the ophthalmologist discharged me from his care. The oral maxillofacial surgery department did the same and the ID consultant referred me to a chronic fatigue specialist and discharged me from his care. This was insane. ‘Common causes of raised neutrophilia are infection and inflammatory conditions.’ [4] Raised neutrophils, along with a collapsed eyelid levitator and a malfunctioning salivary gland, pointed to an obvious cause of infection or inflammation. This was a missed opportunity. Ophthalmology, oral maxillofacial, and infectious diseases, together, could have sorted this.
A well-functioning interdisciplinary team can facilitate a timely and accurate diagnosis and should be leveraged for this purpose.[5]
Patient Despair

Having no diagnosis denies the patient access to correct treatment and leaves the patient feeling not believed. This can lead to feelings of intense despair. When a patient has no diagnosis, they fall into the ‘chronic pain’ territory. ‘Live with the pain’ is the cold rhetoric that accompanies this territory. The lack of care and listening from clinicians has been insulting. No one would keep seeing doctors for 11 years if there was nothing wrong. The medical professionals, who I have seen, know that there is something seriously wrong. Instead of saying, ‘Sorry, we have missed something; we will put this right,’ they close ranks and gaslight me instead.
A Qualitative Exploration

Dr Amelia Barwise conducted a study to understand the ‘organisational, clinician, and patient factors that contribute to diagnostic error and delay.’ The data collected was from 4 hospitals in the Midwest and Southeast of the US. The results of the study showed that many factors contribute to diagnostic error and delay. In addition to cognitive biases of clinicians, organisational and system issues were identified, as well as challenges with interpersonal communication and coordination of tasks. ‘We found delay to be a mostly coordination problem of multidisciplinary teams. Both error and delay are influenced by organisational, interactional, and individual factors.’ [6] Some of the findings, regarding causes of diagnosis error and delay were;
- Organizational and System Factors; Availability of diagnostic tests and demands on clinicians and their time. Lapses in communication with patient about their diagnosis. Reliability of radiology services, especially during the information gathering and interpretation phases. Protocol and bureaucracies stood in the way of acting on diagnostic decisions.
- Interpersonal Factors; Poor communication within the same institution were reported, as was inadequate teamwork.
- Individual Clinician Characteristics; Training, knowledge and experience of clinician, as well as ego, were cited. Cognitive biases of clinicians were a factor and clinicians anchoring to one particular diagnosis, and then not able to switch gears, and think differently.
- Patient Characteristics; Language and cultural barriers were influential. Patient complexity and atypical presentation contribute to diagnostic delay. Vulnerable social groups, are likely to experience diagnostic delay.
Communication and Teamwork

Whilst I appreciate that my clinical presentation has been unusual, I am flummoxed why 4 ID consultants have ignored my raised infection markers. I am equally perplexed why the diagnosis of a soft-tissue infection was not considered a diagnosis back in 2013, when the first ophthalmologist, who I saw, said that ‘the clinical signs all point to infection.’ The data that Dr Barwise found in this study is relevant to my case. Below are some remarks that clinicians made about communication and teamwork. I believe that lack of communication between teams and not acting on clinical evidence are the central causes of my 11-year diagnostic delay.
Communication; “the most common thing I’ve experienced as far as there being an error or delay that has caused significant harm to patients is breakdown in communication …the example I think of is our lab error. So, lab will get a result back that says, this patient’s hemoglobin was 2.5, but we didn’t believe it, so we didn’t tell you about it, and we re-ran the sample instead, and oh, … their hemoglobin’s really 2.5. That one, to me, feels like it’s not that uncommon that you get a call back and say, oh we didn’t believe it. [and repeated it several times].” (FG3)
“…communication between different specialties, I think that is also very crucial. If we don’t communicate appropriately, sometimes we miss things.” (FG9)
“…occasionally, this happens, we see a report, and then the report gets changed without notice. And if you discharge patients without re-verifying the report, that’s disastrous.” (FG8)[7]
Conclusion

I am heartbroken by the time that I have lost seeking a diagnosis for my facial pain. My 11-year diagnostic delay has been avoidable. If doctors had worked together across teams and not consistently ignored clinical evidence, in particular abnormal blood tests, then I would have received a diagnosis years ago. Deep-seated politics between consultants has been a critical component in this delay. Medical professionals have been more intent on listening to one another’s opinions instead of listening to me. As I said in Follow the Leader, in order for things to change, there needs to be a paradigm shift. The ‘there is nothing wrong’ paradigm needs to change to a paradigm of curiosity: ‘What could this be?’ I am concerned, however, that when I do finally receive a diagnosis, it will be too late to treat my condition. My fear is that the damage to the soft tissue in my face and around my head is now irreparable.
When a diagnosis is accurate and made in a timely manner, a patient has the best opportunity for a positive health outcome because clinical decision making will be tailored to a correct understanding of the patient’s health problem.[8]

Foot Notes
[1] What Is Delayed Diagnosis? www.grossmanroth.com
[2] Dr A Barwise et al; What Contributes to diagnostic error and delay? A Qualitative Exploration across Diverse Acute Care Settings in the US, June, 2021, National Library of Medicine.
[3] Suneja M et al; Diagnostic Delays in Infectious Diseases, Jan 2022, National Library of Medicine.
[4] George T, MD and Richards-Chabot D, MD; Assessment of Neutrophilia, October, 2021, BMJ Best Practice.
[5] Dr A Barwise et al; What Contributes to Diagnostic Error and Delay? A Qualitative Exploration across Diverse Acute Care Settings in the US, June, 2021, National Library of Medicine.
[6] Same Author and Source, as Footnote 5.
[7] Same Author and Source as Footnote 5 & 6.
[8] Balogh EP, Miller BT, Ball JR; Improving Diagnosis in Health care, December, 2015, National Academies Press, (US).
Photo Credits; Daniele Franchi, J Balla, J Schiemann, Sam Hogati, Oussema Rattazi, Brett Jordan, Eric Mclean, Julia Taubitz and Harman Sandhu on Unsplash. RDNE Stock project, Pixabay and Daniel Reche on Pexels.

2024-02-15 10:10
On Temporal Arteritis
Disclaimer: This blog post is based on my experiences as a patient. I am on a long-haul journey to find answers and resolution to a chronic condition that I have suffered with for 11 years. I am not medically trained. While I have researched this subject matter carefully, this post does not provide medical advice. If you are suffering from symptoms that you think Temporal Arteritis may be the cause of, then please consult a medical professional.
What Is Temporal Arteritis?
‘Temporal Arteritis (giant cell arteritis) is where the arteries, at the side of the head (the temples,) become inflamed and narrowed. It’s serious and needs urgent treatment.’ [1]Symptoms include a weak pulse, pain at the side of your head (temples,) tenderness on the scalp, and vision problems. Diagnostic tests for Temporal Arteritis are ultrasound of the temple and biopsy of the artery tissue. Corticosteroids are the ‘main modality of treatment, and have been shown to prevent blindness.’ [2]

A woman, suffering from pain with temporal arteritis.
Until 2020, I had periocular pain, around my upper eyelid and around my zygomatic arch. Four years ago, it developed into a pinching pain around my left temple, which now constantly pulsates. I have never experienced pain like it. I have not had my temple pain investigated, nor have I received any answers from ophthalmology about what this pain could be. This blog post asks if a part of my periocular pain, could involve Temporal Arteritis.
My Symptoms
My left temple throbs. The pain shoots all the way around the left side of my head, which gives me a head-ache. My temple is tender to touch, and my pulse is weak on the left side. I have very blurred vision in my left eye. It has been blurred since 2019, following my left superficial parotidectomy, but the blurriness has become more pronounced in the last nine months.
Diagnostic Tests

The blood tests, which doctors use to help diagnose Temporal Arteritis, are; Erythrocyte sedimentation rate, (ESR) and Plasma Viscosity. Both my ESR and Paslma Viscosity have been abnormal. Ultrasound scanning is a diagnostic modality, but according to Muhammed Ameer et al, ‘Temporal artery biopsy is the “gold-standard” diagnostic test for Giant Cell Arteritis, and must always be performed as early as possible.’ [3]I have not had a biopsy of my left temporal artery, nor any ultrasound scanning of my left temple.
The Superficial Temporal Artery

The superficial temporal artery is a terminal branch of your external carotid artery, which is in your neck
I have been learning about the superficial temporal artery, because I wonder whether it may be contributing to the pain around the left side my head and in my ear. The temporal artery supplies blood to your face and scalp. It has multiple branches that pass through the regions in my head and neck, where I experience pain. ‘The superficial temporal artery starts in your parotid gland and runs up and down between your cheekbone and your ear. It branches off into the frontal and parietal branches. Your frontal branch sends blood to your forehead’s muscles and skin. Your parietal branch provides blood to the temporal regions of your head. Other branches of the temporal artery include;
- Transverse facial
- Middle temporal
- Zygomatic-orbital
- Auricular [4]

The arteries of the head in the old book the Human Anatomy Basics, by A. Pansha, 1887.
Reflection

The emboldened words, in the paragraph above, are all the areas of my head and neck, where I am in pain. If my left temporal artery is inflamed, could the pain in my ear, around my zygomatic-orbital area, and around the left side of my head, be caused by an inflamed temporal artery?
It’s Not Adding Up

Something is not adding up between what ophthalmologists are saying, and the level of pain that I am experiencing. I have been to five ophthalmology clinics, at different NHS Trusts, in the UK. A professor of ophthalmology in London, diagnosed my left ptosis, in 2014. He told me that the left levitator on my eyelid had collapsed, and that it needs corrective surgery. But no ophthalmologist has explained what my periocular pain is. They say that there is nothing wrong, but this pain isn’t normal. I am most worried about the pain in my temple. The last ophthalmologist, who I saw a year ago, insisted that it is not Temporal Arteritis, but he refused to do any diagnostic testing, so without doing an ultrasound or a biopsy, how can he be so sure?
Ophthalmologists are excellent at saying what it isn’t, but they never say what it is. Giant Cell Arteritis ‘results from inflammatory changes in the vessel wall.’ [5] So, what else could my temporal pain be, when there has been suspected inflammation and infection in my periocular region for 11 years?
MRI Scans

Radiology Image from an MRI Neck Scan; July, 2022

Radiology Image from an MRI Neck Scan; July, 2022.

Radiology Image from an MRI Neck Scan; July, 2022.
In these radiology images, my left eye does not look healthy. There is visible swelling in the left temporal artery area. When I asked the ophthalmologist about this, he said that it is ‘just the angle plane of the image.’ That doesn’t resonate as true. Something is not adding up about what the ophthalmology world are not saying, and the amount of pain I am in.
Call to Action!

My temporal pain is severe. I have not had a fair hearing from the Ophthalmology world. The last ophthalmologist showed little interest in helping me. The same was true for the Ear Nose and Throat and the Oral Maxillofacial departments, at that NHS Trust. I have received similar indifference from the five other ophthalmology departments in the UK, who I have seen. I am getting a frosty and defensive vibe from my GP practice, who are keeping me at arm’s length. This is a vulnerable predicament to be in, and one that I have been in, for far too long.
The most feared complication of Giant Cell Arteritis is irreversible visual loss caused by ischemic optic neuropathy. Early treatment with corticosteroids can be vision saving.
Muhammed A et al
I do not want to end up with vision loss. This is an urgent call out for any ophthalmologists or oculoplastic surgeons, to please come forward. I will work patiently with you, for as long as it takes to remedy this. You can email me at info@myfacialpain.com, message me directly on my website, or message me on X, @myfacialpain.
Given the risk of irreversible visual loss, treatment with corticosteroids should not be delayed.
Muhammad A et al.

Foot Notes
[1] Temporal Arteritis, www. NHS.uk
[2] Muhammad AA, Peterfry R & Khazeni B; Giant Cell Arteritis (Temporal Arteritis) National Centre for Biotechnology Information, (NCBI.) Copyright © 2024 StatPearls Publishing, LLC
[3] Muhammad AA, Peterfry R & Khazeni B; Giant Cell Arteritis (Temporal Arteritis) National Centre for Biotechnology Information, (NCBI.) Copyright © 2024 StatPearls Publishing, LLC
[4] Superficial Temporary Artery, www.myclevelandclinic.org
[5] Same Author and source as footnote 2 & 3.
Photo Credits: CDD20, Jaron Nix on Unsplash, and Kalz on Pexels.

2024-02-08 09:18
On complicated SSTIs
Disclaimer: This blog post is based on my experiences as a patient. I am on a long-haul journey to find answers and resolution to a chronic condition that I have suffered with for 11 years. I am not medically trained. While I have researched this subject matter carefully, this post does not provide medical advice. If you are suffering from symptoms that you think a soft tissue infection may be the cause of, then please consult a medical professional.
Summary
‘A skin soft-tissue infection, (SSTI) is classified as complicated, (CSSTI) if the infection has spread to the deeper soft tissues. Examples of SSTIs include; cellulitis, diabetic foot infections and surgical site infections. Superficial SSTIs are treated with oral antibiotics. However, complicated SSTIs, (CSSTIs) may require hospitalization, intravenous (IV) antibiotics and/or surgery.’[1]

Methicillin-Resistant Staphylococcus Aureus bacteria, (yellow) interacting with a human neutrophil, (red.)
My previous post asks whether my facial pain could be Facial cellulitis, with secondary lymphatic drainage damage, (lymphoedema.) This post, firstly asks whether I am suffering with an MRSA, complicated SSTI. Secondly, it discusses treatment options for cellulitis, particularly, when the cellulitis has spread to the deeper soft tissues, and has become a complicated soft tissue infection, (CSSTI.) This post examines two effective antibiotics; Linezolid and Vancomycin. These antibiotics are used to treat complicated SSTIs, which are suspected or proven Methicillin-resistant Staphylococcus Aureus bacterial infections, (MRSA.)
Methicillin-Resistant Staphylococcus Aureus, (MRSA) Bacteria

Methicillin-Resistant Staphylococcus Aureus bacteria
In patients with a Penicillin allergy (of which I am one,) the standard antibiotics, used to treat cellulitis are; Clarithromycin, Erythromycin, and Doxycycline. Other alternatives are Metronidazole and Clindamycin, intravenously. All of these antibiotics, minus Clindamycin, have been on repeat prescription for 11 years. They have never eradicated my symptoms, in full. Methicillin-Resistant Staphylococcus Aureus, (MRSA) is ‘a particular strain of the Staphylococcal group of bacteria that resides in the skin. It is resistant to methicillin, the antibiotics, that kills most Staph bacteria. MRSA can lead to Cellulitis.’[2]
‘Given the rising prevalence of MRSA, and the devastating consequences, this organism must be considered when treating patients with CSSTIs.’[3]
My Question

The first Ophthalmologist who I saw in 2014, thought that this was a Staphylococcus Aureus infection. As none of the antibiotics, used to treat cellulitis have worked, it leads me to ask whether I could be suffering with a Methicillin-resistant Staphylococcus Aureus bacterial infection? John Weigelt et al explain in; Linezolid versus Vancomycin in Treatment of Complicated Soft Tissue infections that; ‘MRSA has become a pre-dominant pathogen in many infections, including CSSTI’s. Cephalosporins are commonly used to treat SSTI’s and are effective against MRSA.’[4]Cephalexin is from the Cephalosporin family. Doctors have intermittently prescribed this antibiotic to me over the years. It is one of the most effective antibiotics in taming my facial pain. I also feel better systemically, when I take it, but my symptoms return, when I come off it. This fact adds weight to my question, whether this could be an MRSA bacterial infection?

Methicillin-Resistant Staphylococcus Aureus, (MRSA) Bacteria

Vancomycin
Medics use Vancomycin, intravenously, to treat cellulitis and complicated SSTIs. It is a ‘glycopeptide antibiotic, that has bactericidal activity against aerobic and anaerobic Gram-positive bacteria including, multi-resistant staphylococci.’[5] Weigelt J, et al explain that intravenous Vancomycin has been first-line therapy against MRSA, because other antibiotics, particularly beta-lactams are not active against these strains.
Until recently, therapy for MRSA strains with multidrug resistance has been limited to Vancomycin. New drugs with activity against MRSA have been developed, and Linezolid is one of these agents. [6]
Linezolid

Linezolid is ‘an Oxazolidinone antibacterial, that is active against gram positive methicillin-resistant Staphylococcus Aureus.’[7] It is used to treat complicated skin soft-tissue infections, which are difficult to treat with other antibiotics. John Weigelt and Dennis Stevens, who are both members of the Linezolid Global Advisory Board explain that; ‘Linezolid is a novel Oxazolidinone agent that has a unique mechanism of action whereby it selectively binds to the 50S ribosomal unit and prevents formation of the initiation complex. This action prevents cross-resistance with other antimicrobial agents. Trends favoured Linezolid for MRSA patients and for the overall eradication of Staphylococcus Aureus.’[8]
Weigelt et al, also explain that the 100% oral bioavailability of linezolid allows doctors to avoid the IV route for Linezolid. Doctors, who treat patients for MRSA with linezolid, have found that patients have shorter IV treatment times.
Linezolid versus Vancomycin
Weigelt et al conducted a study, supported by Pfizer inc, which compared Linezolid to Vancomycin in the treatment of Methicillin-resistant Staphylococcus Aureus infections that involved deeper soft tissues, such as cellulitis. ‘Entry criteria included heat/localized warmth, pain/tenderness and a white blood count of 10,000/mm.’ [9]
Methods and Observations

The most common types of infection among the tested group were Cellulitis (46.4%), with 25.8% with skin abscesses and 10.8% with infected ulcers. Patients received Linezolid, 600mg, every 12 hours, IV or orally, or Vancomycin, 1g every 12 hrs, IV. Doctors did clinical observations daily, while the patient was in hospital. They recorded them again, at the long-term follow up on day 35. ‘Patients were judged as cured if complete resolution of all pretherapy clinical signs and symptoms of infection, (e.g.; white blood count) were achieved. Patients were considered improved if two or more of the pretherapy signs and symptoms of CSSTI were resolved, and patients were considered failed if they exhibited persistence of baseline clinical signs and symptoms, or developed new clinical findings consistent with active infection.’[10]
Results

92.2% and 88.5% of patients treated with Linezolid and Vancomycin were clinically cured at the test-of-cure. From the patient population with cellulitis; 92.2% were cured with Linezolid, and 88.5% were cured with Vancomycin. For patients from the clinical population with MRSA infections; 86% (124/140) were cured with Linezolid, and 66.9 % (97/145) were cured with Vancomycin. For patients with MRSA proven cellulitis, the clinical and microbiological outcomes were more successful with Linezolid.
Safety and Tolerability

Patients reported adverse effects with both Linezolid and Vancomycin trials. Some patients, who took Linezolid, reported reactions with their digestive system. Some of the patients who took Vancomycin, reported rash, anaphylaxis and phlebitis.
Study Conclusion

Linezolid outcomes 120/140 patients, (88.6%) were superior to Vancomycin outcomes, 97/145 patients, (66.9%). Weigelt et al explain that the better outcomes among MRSA-infected patients could be related to the skin and tissue penetration of linezolid, or to the inadequate dosing of vancomycin. It is 1g every 12 hrs, for patients with complicated SSTIs. The National Institute for Health and Care Excellence, (NICE) do explain that ‘there are reports, of Staphylococcus aureus with reduced susceptibility to glycopeptides,’[11]which could also be a factor. The result of their study, however, demonstrates that Linezolid therapy is safe, well tolerated, and superior to Vancomycin in the treatment of complicated SSTIs due to MRSA.
Rifampicin and Minocycline
Kotsaki A et al, expand on additional effective treatment for complicated SSTIs due to MRSA. They conducted a clinical trial with hospitalized adults with complicated SSTIs and MRSA. They prescribed the patients oral Rifampicin, 600mg, plus oral Minocycline, 100mg, or oral Linezolid, 600mg for 10 days. 81 patients took Minocycline plus Rifampicin and 42 patients took Linezolid. They found that ‘oral Minocycline plus Rifampicin was non-inferior to oral Linezolid treatment-providing an alternative oral treatment for CSSTI’s.’[12]
I have never tried Minocycline, but a rheumatologist who I saw for two years, prescribed Rifampicin ’empirically,’ for 6 months. I felt much better systemically, when I took it, but it did not subdue my facial pain, significantly.
My Sadness

In Loose Cannon and On Facial Cellulitis, I explain that, an Ophthalmologist, who found clinical evidence of infection, admitted me for 48 hrs of intravenous Ciprofloxacin in 2014. He also prescribed a one-week course of oral Linezolid. He sadly terminated my treatment and discharged me after 48 hrs, with no further observation or follow up. If he had administered IV antibiotics for longer, and kept me under observation, for the 35-day period, that John Weigelt et al explain is necessary, my story may have had a different outcome. His abrupt cessation of my care, however, derailed my recovery. It also initiated a narrative of denial amongst medical professionals, particularly, amongst Ophthalmologists, about my medical condition.
Longer Linezolid?

The one-week course of Linezolid in 2014, was miraculous. The burning in my cheek subsided, and it cleared the pain in my lower eyelid. I was not able to get it again, until 2022. An Infectious Disease Consultant, in Fife, prescribed it to me for one week. That consultant did not carry out any of the recommended observations or follow ups, either. He prescribed it, and then discharged me from clinic. I do not deem issuing a prescription and then closing the case, to be care.
My Frustration

For cyclical antibiotics to be on repeat for 11 yrs; the medical profession, must believe that this is a persistent infection. Clinicians use oral antibiotics to treat superficial SSTIs. This is clearly a complicated SSTI. I cannot understand, therefore, why they will not administer IV antibiotics again, and for longer than 48 hrs. Despite me asking, clinicians have not administered IV antibiotics since my 48 hr admission, back in 2014. It is one of my greatest frustrations, that clinicians have not tried IV Vancomycin, or prescribed Linezolid for longer than one week. I have seen five Infectious Diseases consultants. None of them have answered my question, as to why these antibiotics on repeat, only work in part, and why they will not try IV antibiotics. They will not engage with me past one clinic appointment, which leaves me feeling invisible and unheard.
My Aetiology

Consultants have ruled out cancer. This only leaves infection or inflammation as possible aetiologies. I am certain that This is not chronic pain. My facial pain started as cellulitis, which I am certain, has become a complicated SSTI, (CSSTI.) The last ophthalmologist, who I saw, in November, 2023, said; the issue is with the tissue. He offered no treatment, but his words stand as a useful guide. I want to know if it is possible to get treatment for this potential complicated SSTI, or whether I now have permanent damage, in my soft tissue and masseter muscle.
Consistency of Care

I am seeking a medical professional, who will engage with me past one clinic appointment, and provide me with a diagnosis and prognosis. What is causing this pain? If this is not a complicated SSTI, then, what is it? I want to find a medic, who will explore the option of IV antibiotics, if removing the rest of my parotid gland is out of the question. Due to a delayed diagnosis of 11-yrs, I fear that it may now be too late, for any treatment to work. Time is of the essence, so, can any physicians, who have an interest in complicated SSTIs, please come forward. You can email me; info@myfacialpain.com, contact me via my website, or message me on X, @myfacialpain. Thank you.

Foot Notes
[1] Weigelt J et al; Linezolid versus Vancomycin in Treatment of Complicated Skin and Soft Tissue Infections. Antimicrobial Agents and Chemotherapy, Feb, 2005. Copyright © 2005, American Society for Microbiology.
[2] Matsko, CM; Symptoms of MRSA; Infectious Diseases/ Bacterial Infections, Wikihow.com
[3] Weigelt J et al; Linezolid versus Vancomycin in Treatment of Complicated Skin and Soft Tissue Infections. Copyright © 2005, American Society for Microbiology.
[4] Weigelt J et al; Linezolid versus Vancomycin in Treatment of Complicated Skin and Soft Tissue Infections, Feb 2005, Copyright © 2005, American Society for Microbiology.
[5] Vancomycin; National Institute for Health and Care Excellence, NICE
[6] Same author footnote, as number 1,3 &4
[7] Linezolid; National Institute for Health and Care Excellence, NICE Linezolid | Drugs | BNF | NICE
[8] Weigelt J, et al; Linezolid versus Vancomycin in Treatment of Complicated Skin and Soft Tissue Infections, Copyright © 2005, American Society for Microbiology.
[9] Same Author Footnote as number 8.
[10] Same Author Footnote as number 8 & 9
[11] Vancomycin; National Institute for Health and Care Excellence, NICE.
[12] Kotsaki A et al; Oral Minocycline plus Rifampicin versus oral Linezolid for Complicated skin structure Infections caused by Methicillin Resistant Staphylococcus Aureus; Controlled phase 4 Trial, December 2022, Thelancet.com
Photo Credits: Cottonbro Studio, rdne stock project, Lukas, Artem Podrez and Mateus Souza on Pexels. Julien I, Jessica Pomp, CDC, Wilhelm Gunkel, Sebastiaan Stam and The National Institute of Allergy and Infectious Diseases (NIAID) on Unsplash.

2024-01-30 08:40
On Facial Cellulitis
Disclaimer: This blog post is based on my experiences as a patient. I am on a long-haul journey to find answers and resolution to a chronic condition that I have suffered with for 11 years. I am not medically trained. While I have researched this subject matter carefully, this post does not provide medical advice. If you are suffering from symptoms that you think Facial cellulitis may be the cause of, then please consult a medical professional.
Summary
Cellulitis is ‘an acute bacterial infection of the skin, involving the dermis and subcutaneous tissues.’[1] It is characterised by pain, warmth and swelling. ‘Facial cellulitis is a form of Cellulitis that occurs on the face, typically striking only one side of the face.’[2] This post asks whether my undiagnosed facial pain is caused by Facial cellulitis, with secondary soft tissue and lymphatic drainage damage.

Symptoms and Causation
Symptoms of Facial cellulitis include; swelling of the infected area, abnormal warmth in the face, tight and tender skin, facial pain, chills, fever and weakness. Facial cellulitis is caused when bacteria enter the body through a cut, an open sore, or via an animal or human bite. The two bacteria, which cause this infection are; Group A Streptococci and Staphylococcus Aureus.

Bacteria Staphylococcus aureus on the surface of skin or mucous membrane
‘The situation grows serious, when bacteria, migrate deeper into skin tissues.’ [3]
Complications Of Cellulitis
The main complications resulting from Cellulitis are soft tissue damage and lymphatic drainage damage. Dr Jay Khorsandi, explains in his article on byte.com, that if Facial cellulitis is left untreated, it can spread to the lymph nodes, which can develop into long-term chronic swelling. The infection can also spread to the bones and lymph system, which can lead to low blood pressure. It can also spread to the deeper layer of tissue and fascial lining, and this may eventually damage the lymphatic drainage system, which can also cause long-term chronic swelling; (lymphoedema/angioedema.) Dr Khorsandi makes clear that, without the correct treatment, the bacteria can spread to the neighbouring tissues. ‘If it gets deeper into the tissues, it can cause tissue damage and tissue death.’[4]

Cross section of layers of the human Skin. Adipose tissue with symptoms of Infectious disease. Close-up of Staphylococcus aureus. bacterial infection.
Misdiagnosis
‘Making the correct diagnosis is key to management.’[5]
Sullivan and De Barra explain in Diagnosis and management of cellulitis, that misdiagnosis of Cellulitis is common. ‘Approximately 30% of cellulitis patients are misdiagnosed. Commonly encountered alternate diagnoses include lymphoedema.’ They explain that, positive blood cultures are found in less than 10% of cases, and ‘tissue cultures are negative in up to 70% of cases. Streptococcal A infection is an important cause of culture negative cellulitis.’[6]
Admission to Hospital

In Soft Tissue Infections, Cellulitis, Nottinghamshire Area Prescribing Committee, summarise conditions that lead to a patient needing an urgent hospital admission. These include; if the patient has Class iii cellulitis, has signs of systemic illness, has severe pain, has Facial cellulitis, or has suspected orbital or Periorbital cellulitis. A doctor should admit a patient into hospital if the patient has infection near the eyes, or has an infection that is not responding to antibiotics.
My Causation

This infection started with an opening to the skin, (an insect bite to my lower left eyelid.) My GP immediately diagnosed with me Orbital cellulitis. Straightaway, I had abnormal White Blood Count. This was particularly high with my neutrophils, which have been consistently abnormal for 11 years, (when I am not taking antibiotics.) I have had regular raises with my Red blood count and Haemoglobin count, and when my skin is burning hot, my Mean corpuscular haemoglobin concentration (MCHC) is abnormal. My Erythrocyte sedimentation rate (ESR,) has also been high. These raised blood markers are all indicative of underlying or chronic infection and inflammation. I first consulted with an Ophthalmologist in January 2014. He said, that ‘whilst we may never nail what the bacteria is, Staphylococcus Aureus is the most likely cause.’
My Symptoms

My symptoms are consistent with those of Facial cellulitis. From the outset, I had connected pain and swelling in my cheek and eye. The pain and inflammation spread to the left side of my head, after I applied a steroid eyedrop, called Maxitrol to my eye. I have swelling on the left side of my face, and around my left eye. My skin is burning hot. I have continual facial pain, my skin feels tight, and I often feel weak and tired.
When Things Went Wrong
In January 2014, I had the signs that Nottinghamshire prescribing area say require an admission into hospital. I had diagnosed Orbital Cellulitis, I was systemically unwell, and I was not responding to oral antibiotics. I had tried many rounds of oral Clarithromycin, Erythromycin and oral Doxycycline, (100mg twice daily) but none of these worked. In Loose Cannon, I explain that an Oculoplastic surgeon admitted me for 48 hours of Intravenous Ciprofloxacin, and a one-week course of oral Linezolid, (600mg, twice daily.) The intravenous antibiotics had a therapeutic effect. I felt more energised. They made me feel better. Sadly, having found clinical evidence of infection, the Oculoplastic surgeon kicked me off the ward, and stopped all of my medication, without doing a blood test first, to see if my bloods had normalised.

I had no antibiotics or anti-inflammatory medication for five months. I became severely ill; with pain, boiling hot skin, chills and fever. Knocking on door after door, I eventually found a private clinician, who began empirical treatment. He also kept my bloods under regular observation. If the Loose cannon had continued my care, and given me a much longer round of intravenous antibiotics, I may be in a very different situation today. He has a lot to answer for, not least, an £18,000 bill, that I had to front, to pay for care and treatment privately.
Parotid Gland Anatomy

My parotid gland is a major cause of my facial pain. Investigations and histology reports have found malfunction, reactive lymph nodes, and parenchymal damage (sialolithiasis,) in the gland. As Dr Khorsandi explains, Facial cellulitis can spread to the lymph nodes, and to the deeper layer of tissue and fascial lining. The parotid gland ‘consists of lobules of glandular tissue. The lobules are interspersed with adipose tissue and are covered in a layer of fascia (connective tissue), which forms the parotid capsule. The parotid gland contains superficial and deep lymph nodes. Drainage of these nodes occurs through the deep lateral cervical nodes, primarily the internal jugular nodes, via the infra-auricular nodes.’[7]
Question 1

Soft tissue is effectively what makes up the parotid gland. The parotid gland is also a main source of lymphatic drainage in the face. If I am suffering with Facial cellulitis and it has spread to the lymph nodes and deep tissue in my parotid gland, could this explain my pain and the pathology found? Looking at the anatomy of the gland and how cellulitis spreads deep into the tissue, this seems a possible explanation for my symptoms.
Anatomical Relations
The parotid region is bordered by many significant fascial spaces. It is bordered, as follows;
- Superiorly- Zygomatic Arch
- Inferiorly- Inferior border of the mandible
- Anteriorly- Masseter Muscle
- Posteriorly- External Ear and Sternocleidomastoid. [8]
My Pain
In My Facial pain, I explain that the pain on the left side of my face extends up to the zygomatic arch and into the centre of my cheek. Scans have shown an enlarged masseter muscle. A Radiology report from July 2022, detected abnormality in the retromolar area, which is close to the mandible, and in the buccal fat pad. I also explain in; My Ear Pain that I have severe pain in my left ear; a feeling of fullness/pressure, muffled hearing, and a penetrating pain in the bone behind my ear. I believe this bone is the mastoid space. The CT images do show an enlarged mastoid on the left side, but I have never received an answers about this.
Question 2

I explain in On Parotid Gland Surgery #2 that I the outgoing surgeon has left a lot of my parotid gland remaining. As the gland is bordered with a) the zygomatic arch, which is swollen and painful, b) the mandible and the masseter muscle, where pathology has been found and c) the external ear and the mastoid process, where I have severe and worsening symptoms, is it possible that my symptoms with my left ear and face, are being caused by my remaining parotid gland? If that was fully removed, would that solve my pain elsewhere?
My Periocular Pain

I have acute and persistent pain around my left eye, particularly in the region of my temporal artery. My artery on the left side throbs and it is getting worse. This is the artery, that supplies blood to the eye. I am concerned, as my vision is blurry in that eye. I have no medical care, and the last ophthalmologist who I saw, was dismissive and answered none of my questions. The original diagnosis, in May 2013, was Orbital cellulitis. Is that not then a good reference point to go back to? Is my Periocular pain, chronic Periorbital cellulitis, with secondary Temporal Arteritis?
My Left Sided Head Pain

Brain Anatomy – Temporal Bone
I have unyielding pain around the left side of my head. My head feels soft to touch on the affected side. When I push on it, it makes an indentation, that does not go away for a couple of seconds. I have a stabbing pain at the top of my head. It feels like someone is twisting a cork screw into my head. I have asked four Ear Nose and Throat, (ENT) consultants what this pain could be, but they have provided me with no answers.
Question 3

Dr Khorsandi explains that Facial cellulitis can spread to neighbouring tissues and bones. If Facial cellulitis is the cause of my pain, may it have spread to the soft tissue on my head? Could swelling of the connective tissue that makes up the scalp, be causing my left-sided head pain? Is it possible that potential Facial cellulitis has spread to my temporal bone? Could an enlarged temporal bone be causing my head pain? Or, if the lymphatic drainage is damaged, (Lymphoedema) could my head pain be caused by fluid that has built up in the soft tissue in my head?
My Low blood pressure

I have had low blood pressure during this 11-yr medical episode, but doctors have overlooked these readings. Dr Khorsandi explains that cellulitis can spread to the lymph system and cause low blood pressure. I am wondering whether Facial Cellulitis could be the cause of my low blood pressure? Raised infection markers and low blood pressure are useful clues. It has been very difficult, therefore, when Infectious Disease Consultants disregard this clinical evidence, instead of using it as a compass to find an accurate diagnosis.
Lymphoedema

Human Lymph Nodes Anatomy
In on Lymphoedema, I explain that I consulted with a rheumatologist. He thought that my facial pain and swelling was caused by a soft tissue infection, that has damaged the lymphatic drainage system. This explanation correlates with what Dr Jay Khorsandi says about Facial cellulitis spreading to the deeper layer of tissue and fascial lining, which can damage the lymphatic drainage system, and cause long-term swelling.
Final Reflection

My symptoms are consistent with Facial cellulitis, as are the pathology findings. My final question is, whether I could be suffering with Facial cellulitis, caused by Streptococcal A, or Staphylococcus Aureus, with secondary lymphoedema? Is it possible, that Cellulitis has spread to the deep layers of tissue and fascial lining? And with a delayed diagnosis of 11-yrs, has Facial cellulitis now permanently damaged my facial soft tissue?
I am looking for a microbiologist or Infectious Diseases consultant, who has an interest in complex soft tissue infections, who can diagnose and treat my condition. I am also calling out for Ophthalmologists and Head and Neck surgeons, (ENT or Maxillofacial surgery, who may be able to help. You can reach me via the contact form on my website, by email; info@myfacialpain.com or on X, (formerly Twitter) @myfacialpain.

Foot Notes
[1] Sullivan T & De Barra E; Diagnosis and management of cellulitis, Clinical Medicine 2018 Vol 18. No 2: 160-3, ©Royal College of Physicians, 2018.
[2] Dr Jay Khorsandi; Facial cellulitis: Symptoms, Causes, and Treatment, byte.com
[3] Dr Jay Khorsandi; Facial cellulitis: Symptoms, Causes and Treatment, byte.com
[4] Same source as footnote 2 and 3.
[5] Sullivan T & De Barra E; Diagnosis and management of cellulitis, Clinical Medicine 2018 Vol 18. No 2: 160-3, ©Royal College of Physicians, 2018.
[6] Sullivan S & De Barra E; Diagnosis and management of cellulitis, Clinical Medicine 2018 Vol 18. No 2:160-3, ©Royal College of Physicians, 2018.
[7] Parotid Gland| Complete Anatomy, Elsevier.com
[8] The Parotid Gland – Position – Vasculature – Innervation; Teach Me Anatomy
Photo Credits; Eric W, Pixabay, RDNE Stock Project, and Ann H on Pexels. Lidia Zajdzinska and CDC, and Rohit on Unsplash.
My Tik Tok Videos
@myfacialpain Do you know of a Head and Neck surgeon, who has an interest in benign disease? Please get in touch. #parotidglanddisease #headandnecksurgery #sialolithiasis #parotidectomy #facialpain #facialnervepalsy #delayeddiagnosis #delayedtreatment #medicalhelp #medicalnews
@myfacialpain Ten years, suffering with acute facial pain. 15 NHS Trusts have closed my case. I am on a quest to find answers and medical treatment for my condition. Please contact me if you can help, thank you! #facialpain #newblog #eyepain #earpain #headpain #medicalhelp #medicalnews #delayeddiagnosis #delayedtreatment #chronicillness #invisibleillness

2024-01-17 11:55
Stigma Reduction – A Call For Change
Summary
A Call for Change addresses the urgent need to integrate stigma awareness programs into healthcare settings within the UK. This post concludes this recent series on discrimination, which I believe has been a factor in the 11-year delay, that I have faced getting a diagnosis and treatment for my facial pain. What I have experienced has been horrific. It concerns me how many other patients experience similar barriers to receiving healthcare. I draw on two articles about stigma reduction in healthcare, that give me hope that change is possible. This is a call out to end stigmatization within our healthcare system, to ensure equal access for all.

‘Stigma in health facilities undermines diagnosis, treatment and successful health outcomes. Addressing stigma is fundamental to delivering quality healthcare and achieving optimal health.’[1]
What Is Stigma?
Nyblade et al define stigma as ‘a powerful social process that is characterized by labelling, stereotyping, and separation, leading to status loss and discrimination, all occurring in the context of power.’[2] In their article; Stigma in Health Facilities: Why it Matters and Why we Can change it, Nyblade et al explain that stigma in healthcare facilities manifests in ‘outright’ denial of care, (which I have experienced) provision of sub-standard care, (I have faced this too) and verbal abuse. It also manifests in making people wait longer, or passing their care off to junior colleagues. I have also experienced the latter, at a salivary gland unit in London.

A Consultant referred me to the unit in 2016 for a sialendoscopy procedure. This was to treat obstruction in my left parotid gland. There were three female dental radiologists in the department. They all have a notable reputation for carrying out these minimally invasive procedures. They knew me. At the time of my appointment, the three of them were sitting, eating their lunch in the procedure room. They passed me onto a registrar, who really struggled. She spent an hour trying to get the micro-endoscope into my papilla with a needle and thread. It was grim.
Global Stigma Reduction programs

Nyblade et al identify that ‘common stigma drivers’ in health facilities include negative attitudes, fear, lack of awareness, and lack of knowledge about the condition and the stigma. Their article is a fascinating read. It highlights effective approaches that have been used to reduce health condition stigma in health settings, in countries across the globe. (The UK is not one of the participating countries.) The health condition stigmas include; HIV, Tuberculosis, Mental Illness, Diabetes, Substance Abuse, Leprosy and Cancer. The approaches used were;
- Provision of information; teaching participants about the condition itself and about its stigma and manifestations.
- Skills-building activities, which created opportunities for healthcare providers to develop skills to work with the stigmatized group.
- Contact between healthcare workers and members of the stigmatized group, to humanize the individual and break down stereotypes.
- Structural change looking at changing policies.
They used different methods to deliver these approaches, including; video streaming, lectures, educational materials, interactive learning activities, group work, role playing, discussion, and testimonials. Nyblade et al state that across all of the approaches, staff attitudes and behavioural intent towards stigmatized groups improved.

It is a heartening scenario to hear about the bringing together of health workers with patients who have experienced stigmatisation, into a workshop setting, to share information and increase contact. When I read about these developments, I reflect on my own experiences of stigmatization within a healthcare facility, and I would truly welcome an approach like this within primary and secondary care settings in the UK.
‘Keeping those who are burdened by stigmatization at the centre of any response to stigma has been identified as best practice.’[3]
Future Investment

Nyblade et al conclude that there needs to be future investment in health facility stigma reduction, which should;
- Tackle multiple stigmas at once.
- Focus on empowerment as an approach for health workers to cope with or challenge stigma.
- Target all levels of health facility staff, both clinical and non-clinical.
Mental Health-Related Stigma
‘False beliefs about mental illness can cause significant problems.’ [4]
Knaack et al explain in Mental Illness-Related Stigma: Barriers to Access and Care, that lack of awareness and lack of skills contribute to mental illness stigma-related behaviour. Their article focuses on practical solutions that can be implemented to address ‘embedded’ stigma, in healthcare structures, in relation to mental health. ‘Stigma is a barrier to patient safety through factors such as staff attitudes and institutional culture and the accepted marginalization of mental health patients.’[5]

A survey conducted shows that 53% of medical providers discriminated against a patient from psychiatry. Studies also demonstrate that persons with mental health histories receive poorer quality care for their physical health problems. People with experience of mental health problems, also commonly report that their symptoms are not taken seriously, when they seek care for non-mental health concerns.
Social Contact

Knaack et al argue that culture change is necessary to reduce stigma in healthcare. They state that teaching skills are an effective way to tackle it, as well as hearing first-voice testimonies of peoples lived experiences of both mental illness and experience within the healthcare system. This is referred to as ‘social contact.’ In this case, this is when people with experience of mental illness are seen not as patients but as educators. This contact ‘disconfirms stereotypes, heightens empathy, makes personal connections and improves understanding.’[6] I absolutely love this approach to breaking down barriers between medical professionals and patients.
Myth Busting

The other factor involved in stigma reduction is myth busting, to ‘correct false beliefs that may be negatively impacting care.’[7] Knaack et al state that workshop-based and skills-based interventions and intensive social contact are effective models for myth busting. They describe a 2-hour face-to-face educational program, called Understanding Stigma, which was developed by the Ontario Health Integration Network. It was designed to increase knowledge, skills and awareness, with the aim to change behaviour. Following this workshop, there were ‘Significant improvements,’ re attitudes and behaviour change.
Personal Insight

These stigma reduction programs in Canada, and around the world are inspiring. However, my research has found no equivalent schemes in the UK. Having experienced first-hand, very real barriers to healthcare as a result of stigmatization, I would welcome initiatives like these in the UK. There is no point in having guidance for doctors in Good Medical Practice, stating that a doctor ‘must treat a patient fairly, and not discriminate against them,’ (19) if doctors ignore it, or are simply not given the correct skills and tools to monitor their attitudes and behaviour. There is not enough dialogue about stigma reduction in healthcare. Awareness and skills training would open the door for an inclusive healthcare system, where everyone has equal access to care.

I do not believe that my patient experience is in isolation. I was speaking with a lady recently, who is a full-time carer for a man, who has Down’s Syndrome. The man was complaining of a bad back. The lady took him to the doctor eight times. Each time, the doctor dismissed his problem as ‘cognitive.’ The man ended up collapsing. He is now crippled in a wheelchair. I read similar horror stories on my X, (formerly Twitter) feed daily.

‘Stigma does not only affect those living with stigmatized conditions. Its ramifications reverberate outward through communities. Reducing stigma has the potential to improve the health workplace environment, the quality of care provided by staff, and the clinical outcomes of individuals living with health conditions.’[8]
I Have A Dream

This series concludes with a vision that I have had for many years. The preceding blog series to this one, chronicled an incident with a psychiatrist in Fife, who wrote a discriminatory letter about me, without having met me or speaking to me, which was the precursor to the mental health discrimination that I faced by a surgeon at an NHS Trust in Scotland. In A Psychiatrist in Fife #2, I explain that I heavily researched to see if there were any laws in place, re psychiatrists speculating about patients without meeting them. I found nothing in the UK. I did, however, find The Goldwater Rule, which is observed in the USA. ‘The Goldwater Rule is a statement of ethics issued by The American Psychiatric Association in 1973 It asks psychiatrists to refrain from speculating about the mental state of public figures, without formally evaluating them.’[9]

This incident with the psychiatrist in Fife was horrific. It was traumatising. A surgeon both victimised and ghosted me, as a result of it. I do not want another patient to ever experience such a violation. My dream is to see The Goldwater Rule observed in the UK. My dream is to see it applied, not only to public figures, but to everyday people, like me and you.
Change Must Come

The updated edition of Good Medical Practice comes into effect on January 30, 2024. I was glad to see that it has an addition to Domain 3: Colleagues, Culture and Safety, which states that a doctor ‘must not present opinion as established fact,’ (89 d.) This is encouraging! If this had been GMC guidance, in 2020, when this incident with the psychiatrist occurred, I could have proven a breach of GMC guidance by the psychiatrist, and there may have been a different outcome to my GMC complaint. Change must come. There needs to be stringent reform to ensure that everybody has equal access to care. Stigma must no longer present as ‘a barrier to care for people seeking services for ‘disease prevention and treatment of acute and chronic conditions.’[10]

Foot Notes
[1] Nyblade,L at al; Stigma in health facilities: why it matters and how we can change it, BMC Medicine, 2019.
[2] Nyblade, L et al; Stigma in health facilities: why it matters and how we can change it, BMC Medicine, 2019
[3] Same source as footnote 1 & 2
[4] The Mayo Clinic: Mental Health: Overcoming the Stigma of Mental Illness.
[5] Knaack S et al: Mental Illness-Related Stigma in Healthcare: Barriers to Access and Care and Evidence-Based Solutions.
[6] Knaack S et al: : Mental Illness-Related Stigma in Healthcare: Barriers to Access and Care and Evidence-Based Solutions.
[7] Same Source as Footnote 5 & 6
[8] Same Source as Footnote 5,6 &7
[9] The Goldwater Rule. Psychology Today.
[10] Nyblade L et al: Stigma in Health Facilities: Why it Matters and How We Can Change It, BMC Medicine, 2019
Photo Credits; Clem Onojegkwo, Jason Rosewell, Topshere Media, National Cancer Institute, Ehimetalor Akhere Unuabona, Nathan Anderson, Jason Goodman, Morgan Basham, Florida Memory and Chris Barbalis on Unsplash. Pixabay, Matheus Bartelli, Henri Mathieu Saint Laurent, Karolina Grabowska, Mart Production and Demeter Attila on Pexels.

2024-01-04 04:48
On Mental Health Discrimination #2
Summary
On Mental Health Discrimination #2 discusses discrimination that I experienced at an NHS Trust in Scotland, within the context of The Equality Act, 2010, which is a law that protects a variety of people from discrimination. This blog post focuses on the aspects of The Equality Act, which speak about the responsibility of providers of services, like hospitals, to not discriminate against anyone, and the obligations set out in The Public Sector Equality Duty.

Ghosted
I was ghosted by a Head and Neck surgeon for 18 weeks. After seeing me once, and promising to ‘get me back to find a way forward,’ he ignored me for over 4 months, and then closed down my case. He did not provide me with any explanation why. He left me with no medical care. His conduct was motivated by what seems to have been Mental Health Discrimination. I was denied medical treatment for my facial pain, because of stigmatization.

The Equality Act, 2010
Chapter 1 of The Equality Act, 2010, sets out that the following characteristics, are all protected characteristics from discrimination;
- age
- disability
- gender reassignment
- marriage and civil partnership
- pregnancy and maternity
- race
- religion or belief
- sex
- sexual orientation.[1]

Prohibited Conduct
Chapter 2 of The Equality Act, 2010 sets out what Prohibited Conduct is, regarding these protected characteristics;
- Direct discrimination; This is if person A discriminates against person B because of a protected characteristic, and if A treats B less favourably than A treats others.
- Discrimination arising from a disability; This is when person A discriminates against a disabled person, and treats them unfavourably because of something arising as a consequence of their disability.
- Indirect discrimination; This occurs if person A discriminates against person B, and applies a provision to person B, which is discriminatory in relation to one of B’s protected characteristics.
- Vital to my experience, is the subsection to this clause, which states that a provision or practice is discriminatory if; (a)person A applies, or would apply, it to persons with whom person B does not share the characteristic, (b)it puts persons with whom B shares the characteristic at a particular disadvantage when compared with persons with whom B does not share it, (c)it puts, or would put, B at that disadvantage, and (d)A cannot show it to be a proportionate means of achieving a legitimate aim. [2]
- I have italicized person B, not sharing the characteristic because the surgeon discriminated against me, by saying in his note to the radiologist to; ‘be careful with this one,’ because, he said ‘I have ‘significant psychiatric problems,’ which I do not have. I do have other restrictions, such as mobility, but, in this case, I do not share the characteristic of disabled.
The Provision of Services

The Equality Act protects you from discrimination in a number of places; at work, in education, when buying or renting property, and using services, such as hospitals, restaurants and leisure centres. These can be free services or ones that you pay for. Because I experienced both direct and indirect discrimination, at an NHS Hospital, and by a doctor, I am going to focus on part 3 of The Equality Act, 2010, which is; The Provision of Services and Public sector Equality Duty. The Equality Act states;
‘A Service Provider concerned with a provision of a service to the public, must not discriminate against a person requiring the service, by not providing the person with the service. 2. A Service provider must not, in providing the service discriminate a person by a) terminating the provision of the service, or b) by subjecting person B to any other detriment. A service provider must not victimise a person requiring the service, by not providing the person with a service. In providing the service, the service provider must not victimise the person by a) terminating the provision of the service or b) subjecting the person to any other detriment.’[3]
Public Sector Equality Duty

Organisations that are public authorities also have special legal obligations under the public sector equality duty. The Equality Act states that; A public authority must, have due regard to the need to a) eliminate discrimination, harassment, victimisation, and b) advance equality of opportunity between persons who share a relevant protected characteristic and persons who do not share it. Additionally, chapter 1, part 2, section 149 of The Equality Act states that there is a need to a) tackle prejudice and b) promote understanding, to be able to ‘foster good relations between those who share a protected characteristic, and those who don’t.’[4]
Conclusion
The incident that took place at an NHS trust in Scotland, where a Head and Neck surgeon wrote a discriminatory comment about me to a radiologist, refused to discuss my scan results with me, ignored me for 18 weeks, did not provide me with a follow up consultation, did not reply to my letters, and closed my case, was a potential breach of The Equality Act. The surgeon terminated my care due to ‘seeming’ discrimination, which caused me sustained and severe detriment. During the time that he was stonewalling me, my ear pain and facial pain grew worse. I developed acute Pulsatile Tinnitus in my left ear, and I had no medical care. It was horrific. My experience of being victimised by him, was akin to torture.

vector illustration of diagram of human ear anatomy
This discriminatory incident happened under the roof of a public authority; an NHS hospital. The NHS Trust therefore failed to follow the public sector equality duty, and eliminate discrimination and victimisation. A member of staff, higher up, in management, should have caught this mental health discrimination. The surgeon should have been challenged about what he wrote about me, in his memo, to the radiologist.

Foot Notes
[1] The Equality Act, 2010, Chapter one.
[2] Part 2, Chapter 2, Discrimination, Section 19; Indirect Discrimination; The Equality Act, 2010 (legislation.gov.uk)
[3] Part 3; Services and Public Functions. 29; Provision of Services. The Equality Act, 2010 (legislation.gov.uk)
[4] The Equality Act; Chapter 1, Part 2, Section 149; Public Sector Equality Duty Equality Act 2010 (legislation.gov.uk)
Photo Credits; Usman Yousaf, Luis Melendez, CDC, Alexander Grey on Unsplash and Plato Terentev on Pexels.

2023-12-04 09:13
On Mental Health Discrimination #1
Summary
‘There are different ways you can experience discrimination including: direct discrimination: if you’re treated worse than others because of your mental health problem and indirect discrimination: if a person or organisation has arrangements in place that put you at an unfair disadvantage. Mental Health Discrimination also includes if you’re harassed, intimidated, or humiliated.[1]

In A Psychiatrist in Fife #1, I recount an incident that occurred with a psychiatrist in Scotland, who had never met me, who wrote a letter about me, saying that I have Factitious disorder and that my facial pain is ‘made up to fill a need to be sick.’ As a result of this letter, I was unable to get medical treatment for a physical condition. In this post, I discuss an incident of both direct and indirect mental health discrimination, that I faced as a result of this letter, which further delayed my ability to get a diagnosis and medical treatment for my facial pain.
Mental illness related stigma within the healthcare system, creates serious barriers to access and quality care. [2]
How It Happened

The Ear Nose and Throat consultant in Fife, who informed me about the psychiatrist’s letter, referred me to a Tertiary Head and Neck Centre, because an MRI scan had shown abnormal masseter muscle. However, he included the psychiatrists’ letter with his referral. The next surgeon told me, that he thought the psychiatrist should not have written the letter, without meeting me, and he agreed to do an MRI Neck and CT Neck scan. He told me that, after the scans, he would get me back to ‘find a way forward.’
In On Good Medical Practice #2, I discuss the ways in which one of the surgeons who I consulted with, deviated from Good Medical Practice. It was this surgeon. I never heard from him again after the initial consultation. He sent me for the scans, but he did not offer me a follow up consultation to discuss the results. I wrote to him four times asking for a follow up consultation, but he ignored my letters. I was stonewalled by him for eighteen weeks.
Closed Case

My left ear pain was intensifying. I had a feeling of fullness and violent Pulsatile Tinnitus in my left ear. I explained this to him in written correspondences, but he continued to rebuff me. The surgeon closed my case. I later discovered that it was mental health discrimination, that seemingly lay behind his silent treatment of me.
My Discovery
I wrote to the NHS Trust and requested copies of my MRI and CT scans. Two CD disks and two radiology reports arrived. When I studied the contents, my disbelief was hard to contain. I was stunned to see in the CT Neck and CT Bone scans such a stark asymmetry between the two sides of my face. There were also large dense white areas, where I experience the pain. I was unable to ask the surgeon any questions, due to him ghosting me. More startling, however, was seeing in the report, what the surgeon had said about me to the radiologist. He wrote;
Be Careful with this one. Patient has significant psychiatric problems but also chronic pain from parotid disease. Also, previous story of orbital cellulitis and pain across the head.

This surgeon had met me once, for 30 minutes. He took that information from a letter written by a psychiatrist, who had never met me, which the surgeon himself, had said was wrong. This was beyond shocking. This was a Head and Neck scan being requested for physical pain. It was therefore grossly inappropriate to a) remark about my mental health and b) present inaccurate information and opinion as fact. The surgeon’s remark clearly influenced the radiologist, who seems to have not been transparent, in his reading of these radiology images.
The Reality
The radiology images below, are from the scans that this surgeon requested. Dear reader; I have left sided facial pain. Does the asymmetry between the two sides of my face look like a physical or a psychiatric problem?
Radiology image from CT Neck scan, with contrast. July 2020.

Radiology Image from CT Neck Scan, with contrast. July 2020.

Radiology Image from a CT Neck Scan, with contrast. July, 2020.

Radiology Image from CT Neck Scan, with Contrast. July, 2020.

Radiology Image of CT Neck Scan, With Contrast. July, 2020.

Radiology Image from CT Neck Scan, With Contrast, July, 2020.

Radiology Image from CT Bone Scan. July, 2020.

Radiology Image from CT Bone Scan. July, 2020.
Radiology Image from CT Bone Scan, July, 2020.
I do not have ‘significant psychiatric problems.’ My current episode of acute distress, and yes, protracted crisis, is related to enduring severe physical pain for now eleven years, and not being shown an ounce of respect by over fifty medical consultants. It would take its toll on anyone. The picture of the man’s face below. That is how I feel inside. It’s not a psychiatric problem. It’s a human who has been kicked hard by the system and who is well and truly beat.

Even if a patient does have ‘serious psychiatric problems,’ this comment has no place on a radiology request form for a CT Neck scan, which is investigating parotid disease. No place at all. The surgeon’s discriminatory remark is now on my Scottish medical records. If a radiologist from another NHS Trust requests these scans, they will see it. A new radiologist has already requested those scans from Scotland, and I am certain that he has seen the surgeon’s comment. This recent radiologist has admitted to finding abnormality in my recent MRI scan, but no follow up, or treatment has been offered. They have closed my case again.
Diagnostic and treatment overshadowing, whereby physical symptoms are misattributed to a patient’s mental illness, creates delays in diagnoses and treatment options.29’ [3]
Good Medical Practice

Domain 2- Patients, Partnership and Communication
‘The approach and attitude of a medical professional can have a lasting impact on a patient. Treating patients with kindness, compassion and respect can profoundly shape their experience.’
Treating Patients Fairly and Respecting their Rights
19) You must treat patients fairly. You must not discriminate against them or allow your personal views to affect the treatment that you provide.
Sharing Information with Patients

29) You must listen to Patients and encourage an open dialogue about their health and respond honestly to their questions.
Domain 4- Trust and Professionalism
Communicating as a Medical Professional
All Professional Communication
89) You must make sure any information you communicate as a medical professional is accurate, not false or misleading. This means;
a) You must take reasonable steps to check the information is correct.
d) You must not present opinion as established fact.[4]

Ignoring me for eighteen weeks, not answering my questions, and writing a misleading and inaccurate comment about me to another medical professional, in which he presented his ‘opinion as fact,’ (89 d) is not following guidance. This surgeon discriminated against me in a vulgar way. This is not ‘treating a patient fairly,’ (Good Medical Practice,19.)
As I said in Good Medical Practice #3, My Facial Pain is a quest to find a diagnosis and medical treatment for my condition. It is also a quest to understand how such poor conduct by medical professionals has gone unregulated for this long. Why has no one intercepted this bad practice? It is a disgrace. There needs to be much stricter regulation of all doctors in the UK.

‘The combination of high rates of physical illness and low rates of receiving effective treatment leads to fatal consequences of discrimination and neglect.’[5]
Systemic Discrimination

I have always supported anti-discrimination movements, particularly anti-sexism and discrimination against people of other races, but until you actually experience discrimination for yourself, it is not possible to understand how widespread and enduring its effects are. A lady on X, (formally Twitter) recently replied to one of my tweets about institutional bullying. I get this… she said. Institutional bullying has an entrenched power far beyond that of individuals.

That applies to systemic discrimination, too. The ‘note’ that the Head and Neck surgeon wrote to the radiologist, saying that I have ‘significant psychiatric problems,’ was yes, written by the surgeon, but it was not his voice in isolation. It was the NHS Trusts’ voice too. That opinion has the power to spread from that NHS Trust to another. It then develops into an all-pervasive belief about you, which becomes entrenched within the system. It’s petrifying. I felt backed into a corner with no where to turn.
I felt unable to speak for fear of saying something that would compound this discriminatory view of me.

Qualitative research has found that for many healthcare providers, it is only through the experience of receiving anti-stigma training that they become aware of the subtle and unintended ways certain beliefs and behaviours may have been contributing to stigmatizing experiences among their patients. (Knaak et al.14 see also Sukhera et al.25 and Horsfall et al.28) [6]

Foot Notes
[1] The Mental Health Foundation. Stigma and Discrimination, www.mentalhealth.org.uk
Stigma and discrimination | Mental Health Foundation
[2] Knaak S, Mantler E, Szeto A; Mental Illness-Related Stigma in Healthcare, Healthcare Management Forum, March, 2017.
[3] Knaak S, Mantler E, Szeto A; Mental Illness-Related Stigma in Healthcare, Healthcare Management Forum, March, 2017.
[4] The General Medical Council; Good Medical Practice 2024, published August 2023. This revised edition of Good Medical Practice will come into effect on January 30, 2024
[5] Thornicroft G, Rose D, Mehta N; Discrimination Against People with Mental Illness: What Can Psychiatrists Do? Cambridge University Press, January, 2018. Copyright © The Royal College of Psychiatrists, 2010.
[6] Knaak S, Mantler E, Szeto A; Mental Illness-Related Stigma in Healthcare, Healthcare Management Forum, March, 2017.

2023-11-27 09:13
A Psychiatrist In Fife #3
Summary
This post concludes a series about a ruinous incident that occurred with a psychiatrist, who wrote a letter, without meeting me or speaking to me, which claimed that I have ‘Factitious Disorder,’ and that my facial pain is ‘fictionalization.’ He published this letter on my medical records. I discuss the devastating impact that this incident had on me personally, and the response that I received from The General Medical Council to my complaint about this psychiatrist and his actions.

Fitness to Practise

The General Medical Council, (GMC) only investigates complaints about doctors, whose fitness to practise is in question.
‘Doctors have a respected position in society. Their work gives them privileged access to patients, some of whom may be very vulnerable. A doctor whose conduct has shown that they cannot justify trust placed in them should not continue in unrestricted practice. The public is entitled to expect that their doctor is fit to practise and follows our principles of good practice described in Good Medical Practice.
Most doctors measure up to these high standards, but a few seriously fall short and put patients at risk, cause them serious harm or distress, or undermine public confidence in doctors. For that reason, we have legal powers to take action.’[1]
GMC Regulation

The General Medical Council are unlikely to indicate a fitness to practise problem with one-off mistakes. ‘It is serious or persistent failures to follow guidance that will put a doctor’s registration at risk.’[2] The behaviour which could call a doctor’s registration into question are;
- A doctor’s performance has harmed patients or put them at risk of harm.
- A doctor has shown a deliberate or reckless disregard of clinical responsibilities towards patients.
- A doctor’s health is compromising patient safety.
- A doctor has abused a patient’s trust or violated a patient’s autonomy or other fundamental rights.
- A doctor has behaved dishonestly, or in a way to mislead or harm others.
My Complaint
My complaint to the General Medical Council was that this psychiatrist wrote a discriminatory letter, without having met me or spoken to me, which led to me being refused medical treatment for my facial pain. I complained that his letter was misleading, and breached Good Medical Practice, (71 and 71a.) The psychiatrist defended his actions with a brazen argument, claiming that he wrote this letter ‘to keep me safe.’ Keep me safe?

It didn’t keep me safe. It pushed me to the edge of the cliff.

The GMC opened a provisional enquiry. They obtained further information to see if the case required a full investigation, or whether it could be closed down. From the information they acquired, they did not find this psychiatrist unfit to practise.
The psychiatrist had apparently acquired the info that I had ‘factitious disorder’ from my notes. During a two-week admission on a psychiatric ward, (which I had requested,) the locum psychiatrist on the ward, who I saw only twice, said that he thought that I had Factitious Disorder. This psychiatrist took that information from my notes. However, what the GMC missed was, that he wrote this letter without arranging an appointment with me first, to ‘check that the information was correct,’ (Good Medical Practice, 71a.) A warning should have been given to him, to take greater care, re diagnosing patients without meeting them.
What was shocking, was how the GMC manipulated my complaint to support their argument. In their outcome report, they said that I had complained that the psychiatrist had written the letter, without looking in my records/notes. I did not say this. I complained that he had written it without meeting me. The GMC twisted my words to support their defence of the psychiatrist’s actions. I didn’t appreciate being manipulated like that.

Protecting Public safety?

The role of the GMC is to protect public safety. However, I do not feel that they have protected patient safety on this one. This psychiatrist did a) show reckless disregard of clinical responsibilities towards me, b) he violated my autonomy and two of my human rights (fundamental rights) and he c) behaved dishonestly, and in a way designed to mislead others.
By the GMC choosing to defend the psychiatrist, he will likely cause another patient immeasurable harm in the future. That is not protecting public safety. It is protecting the actions and status of a crooked doctor. However, being silenced by a supervisory body is tough. It is impossible to challenge their decision, even with the anomalies.

Twist

The manner in which the GMC twisted what I had said, is consistent with my experiences of complaining to supervisory bodies. My know-how of complaining to regulatory bodies, like NHS England and The Parliamentary Health Service Ombudsman, (PHSO), is that they will often bend the tenet of the complaint, to protect the big guy. Quashing the little guy, who has no power, is easier than standing up to a bully, who has an army of defence behind him.
The System
In On Shame, I said that the system is broken. The fact that I am suffering with unrelenting facial and orbital pain, for which I cannot get treatment, is torturous enough. For there to be a letter on my Scottish medical records, written by somebody who has never met me or spoken to me, which claims that I am ‘making all this up to get attention to feed the need for a sick role,’ which no professional has questioned, and which the General Medical Council has excused, makes the system, not broken, but rotten to the core.

Impact

This letter nearly killed me. By writing these incriminating words, this psychiatrist closed any treatment doors that I had opened, by the courageous act of moving to Scotland. Things were going well. My GP had referred to Ear, Nose and Throat. He believed me. However, after this letter was published, I was looked upon as filth by the medics. He backed me into a corner. I had no room for manoeuvre. This incident pushed me into an acutely fragile state, and if it had not been for the support of the charitable sector, I would not have made it.

Coward

This psychiatrist left the position as locum psychiatrist, three months after he published this letter about me. He planted an explosive. He watched it explode, but he didn’t stick around to clear up the mess. I faced obscene mental health discrimination from medics as a result of his letter, and the fact that he was nowhere to be seen when hell broke loose, was a shameful act of cowardice.

Leaving Fife

As soon as the second lockdown lifted, I scarpered. Before leaving Scotland, I telephoned my GP Surgery, to find out if they had entered Factitious disorder onto my medical summary. Thankfully, because the psychiatrist had never met me, and I had received no psychiatric assessment, they had not entered it under any of my diagnoses. Factitious disorder is not on my medical summary in England either. Even though, now that I am back in England, this discriminatory letter has no power over me, I want it removing from my Scottish records on principle. I do not have Factitious Disorder, or any such disorder. This letter, therefore, has no place, on any of my records.
On Trauma

I experienced trauma, both as a child and teen. My experience of trauma is that gradually, over time, it softens, and has less hold over you. However, the shock of this incident has not thawed. It still feels as raw as it did when it happened, three years ago.

I lived in San Francisco during my twenties. Minor earthquakes, that don’t reach the headlines, regularly occur there, because it is situated close to The San Andreas Fault. After the tremor, parts of the landscape; trees, fences, lampposts, may change shape. That damage never repairs.

Since the day that the ENT consultant told me about this bigoted letter, something within my inner architecture has dented. I am on constant high alert and constantly looking over my shoulder. This incident has charred my trust, and I am not confident that this will ever heal.

Betrayed

I know the terrain of abuse and betrayal well. My parents consistently busted my boundaries. As a consequence of their behaviour, many others walked all over me until the age of 30, when I made a difficult decision to walk away from many significant relationships.
My parents were damaged people, but there wasn’t the access back then to the psychological therapies that there are now. However, this psychiatrist was not ill. He made a dangerous judgement about me as a person, without meeting me, which he has published on my records, and which adversely affected how medics viewed me.
My mother may have failed me in many ways, but what she couldn’t provide with affection, money, or possessions, she imparted with extraordinary values. She raised me to honour fairness, resourcefulness and honesty. This psychiatrist has not only undermined my integrity, but he has insulted my late mother’s legacy, which makes this, by far, the worst betrayal that I have ever experienced.
A Tribute

I want to pay tribute to the non-statutory organisations who supported me through this catastrophic incident and the consequences that ensued from it. A heartfelt thanks goes to The Bethany Christian Trust, (Housing Support, Fife) and Breathing Space; the national helpline in Scotland.
I was treated as less than human by the statutory services in Fife. They kicked me lower than I thought it humanly possible to fall. Thank you for the respect and dignity that you showed me. Your kindness helped me to find fleeting moments of self-worth in a period of darkness and chaos. The work that you do in society is heroic. On behalf of myself, and the thousands of vulnerable people, whose lives you touch, enrich and save– thankyou.

Foot Notes
[1] The General Medical Council; The Meaning of fitness to practise, February, 2021, www.gmc-uk.org
[2] The General Medical Council; The Meaning of fitness to practise, February, 2021, www.gmc-uk.org
Recommended Articles

2023-11-15 01:49
A Psychiatrist In Fife #2
Summary
A psychiatrist in Fife #2 follows on from my previous post, in which I discuss a discriminatory incident that occurred with a psychiatrist, who had never met me or spoken to me, and who wrote a letter, claiming that my facial pain is fictionalization. He sent this letter out to multiple agencies. The unfounded letter profoundly affected how I was viewed by medics in Scotland. This post discusses the ethics around the issue of psychiatrists evaluating a patient without meeting them, and what actions I took to challenge this discriminatory incident.

My Primary Action

I discovered that this psychiatrist was acting as a locum psychiatrist for the local mental health team in Fife. I immediately withdraw from the mental health services there. It was too dangerous to remain open to a team, who had a leader at its helm, who was this perilous. I had to withdraw to prevent anymore discriminatory letters being published about me. I relied, instead on the wonderful help of the non-statutory support sector.
Sci Gateway

It was terrifying residing in a country with this discriminatory letter on my file, because it was visible to any professional who logged into my medical records. Sci Gateway is the national system in Scotland that integrates primary and secondary care systems. In England, when you go to see a consultant, unless they really root around, the only information in front of them is the GP referral, and any investigations done at that hospital. In Scotland, the consultant has both your secondary care and GP records in front of him. I wanted to leave Scotland, but I couldn’t, due to the national lockdown.

Good Medical Practice 1

Good Medical Practice States that a Doctor Must;
Treat Patients and Colleagues Fairly and Without Discrimination
59) You must not unfairly discriminate against patients or colleagues. You should challenge colleagues if their behaviour does not comply with this guidance, and follow the guidance in paragraph 25c (see section Domain 2: Safety and quality) if the behaviour amounts to abuse or denial of a patient’s or colleague’s rights. [1]
(Paragraph 25c – If you have concerns that a colleague may not be fit to practise and may be putting a patient at risk, you must ask for advice from a colleague, your defence, or us.)
Good Medical Practice 2

Good Medical Practice States that a Doctor Must;
Act with Honesty and Integrity
71) Be honest and trustworthy when writing reports, and when completing or signing forms, reports and other documents. You must make sure that any documents that you write or sign are not false or misleading.
a) You must take reasonable steps to check the information is correct. [2]
This letter, written by the psychiatrist, is a radical departure from Good Medical Practice. It is not honest or trustworthy. He has written and signed an extremely misleading document, that led to me being denied medical treatment for my facial pain because of it. He didn’t take ‘reasonable steps to check that the information is correct.’ That would have involved him meeting or speaking with me, which he didn’t do. Good Psychiatric Practice, which sets out standards of practice for psychiatrists, ‘is aligned to the General Medical Council’s (GMC’s) Good Medical Practice, the standards for all medical practitioners.’[3]
My GP and the Community Psychiatric Nurses, neither complied with GMC guidance. They all knew that what this psychiatrist had said about me in his letter was not true. They also knew that his actions had both caused me harm, and not followed guidance. None of them, however, challenged it, as advised above in point 25c. They stayed quiet, and turned away from me. It bloody hurt.

A Canadian Optician

I came across a case in Canada, where a psychiatrist had written an evaluation about an Optician, without meeting him. The Opticians College had requested this evaluation. I found out that the psychiatrist’s determinations were reached by a review of the optician’s emails to the college. The Optician reported the psychiatrist to the Medical Regulator in Canada, who concluded that the psychiatrist’s conduct was ‘appropriate.’
If the Canadian regulator found the actions of that psychiatrist ‘appropriate,’ then the UK equivalent; The General Medical Council, would likely conclude the same thing for my case. The term ‘appropriate’ acts as an umbrella under which supervisory bodies appear to excuse and defend poor conduct. The parameters of the term are wide and lenient. I was not therefore, hopeful about reporting my grievance to the General Medical Council.
The Goldwater Rule

The Goldwater Rule, which is observed the USA, asks psychiatrists to refrain from diagnosing a person without meeting and examining that person as a patient.
The Goldwater Rule is a statement of ethics first issued by the American Psychiatric Association in 1973 restraining psychiatrists from speculating about the mental state of public figures. The rule enjoins psychiatrists from professionally diagnosing someone they have not personally evaluated.
Psychology Today
The activating force behind The Goldwater Rule was during the Presidential campaign in 1964, when Senator Barry Goldwater was running against President Lyndon Johnson. FACT magazine, solicited and published psychiatric opinion about Barry Goldwater, which proved highly embarrassing for the field of psychiatry.
Reflections

From the research that I did into the legalities of what this psychiatrist had done, I found that his damning letter that he had written about me had definitely breached Good Medical Practice, and it was possibly a breach of two of my human rights. However, there was no rule or law in the UK that says it is illegal to diagnose a patient without meeting them. Unethical? Definitely yes. But, illegal? Unfortunately, not. Not in the UK, anyway.
General Medical Council Complaints

The General Medical Council, (GMC) is the national regulatory body for doctors who are registered in the UK. Their role is to protect public safety and uphold public confidence in the medical profession. The GMC only deal with serious complaints about doctors, that might require a doctor’s registration to be restricted or removed. They don’t get you an apology or a review of your case. They look at a doctor’s fitness to practice.

The GMC will investigate complaints about; ‘1) serious mistakes in carrying out medical procedures, 2) failure to examine a patient properly, 3) fraud or dishonesty, 4) discrimination, 5) serious breaches of a patient’s confidentiality, and 6) any serious criminal offence.’[4] If the GMC finds a doctor unfit to practice, they can issue the doctor a warning, agree for the doctor to retrain or refer the doctor to a tribunal. The tribunal can decide to a) put conditions on a doctor’s registration, b) suspend the doctors name from the register, and c) remove the doctors name from the register entirely.

I questioned whether my complaint about this psychiatrist was serious enough for the GMC to consider. The Citizens Commission on Human Rights thought that it was, and they kindly wrote me a letter of support. I sent in a concern to the GMC, on the grounds of discrimination. The tenet of my complaint centred around the fact that the psychiatrist had written a discriminatory letter about me, without meeting or speaking to me.
The Triage Stage
The General Medical Council triage team asked to see a copy of the psychiatrist’s ‘alleged’ letter. I hadn’t actually seen it myself. I requested a copy from my GP. When I read the contempt with which he spoke about me, I felt dirty. I stood in the car park of my GP Practice in complete disbelief.

The psychiatrist did admit in the opening sentence of his letter that he had never met me, but the shock, was the condemning tone of his letter, and the agencies that he had copied in. I felt deeply humiliated. He also made a comment about a recent MRI scan of mine. He was a locum psychiatrist. It wasn’t his role to comment on radiology data.
Provisional Enquiry

The General Medical Council, (GMC) decided to open a Provisional Enquiry into the psychiatrist’s actions. ‘A provisional enquiry involves obtaining targeted information to help inform a decision about whether the concern raised amounts to an allegation that a doctor’s current fitness to practise is impaired and therefore requires a full investigation. It is limited to gathering one or two discrete pieces of information.’ [5]
The GMC applied for my notes from the psychiatric ward where I stayed for two weeks. They told me that they would write to the psychiatrist, and that they would be informing his Responsible Officer about the complaint. This was an encouraging start, but I was not hopeful about a positive outcome. The GMC were already using words like ‘acceptable,’ and ‘appropriate.’ The definition of those terms, within complaints processes, is murky. I wasn’t under any illusions.
GMC Victim Support Service

The General Medical Council’s (GMC)Victim Support Service offers a 24-hour helpline for anyone who has an investigation or Provisional Enquiry open about a doctor. It provides support re the investigation process. I received nine months of support from the GMC Victim Support Service. I was assigned a wonderful worker, who phoned me weekly. Their support helped me to process the shock attached to this violation. It is a wonderful service. They truly understand how it feels to be a victim of abuse of power. I am extremely grateful to the GMC Victim Support service, for the time and space that they gave me, to process this violent attack on my integrity.

Foot Notes
[1] The General Medical Council; Good Medical Practice, March, 2013, www.gmc-uk.org/guidance
[2] The General Medical Council; Good Medical Practice, March, 2013, www.gmc-uk.org/guidance
[3] The Royal College of Psychiatrists; Good Psychiatric Practice, 2009.
[4] The General Medical Council; How To Raise a Concern about a Doctor, www.gmc-uk.org
[5] The General Medical Council; Guidance for Decision Makers on Provisional Enquiries, www.gmc-uk.org
Recommended Articles
The GMC- Our Role In Protecting The Public.
How To Raise A Concern About A Doctor
An Introduction to Clinical Ethics in Psychiatry
Is It Ethical For Doctors To Diagnose Patients They Haven’t Examined?

2023-11-04 12:03
A Psychiatrist In Fife #1
This blog post contains wording about suicide that some people may find triggering. If you need support, and you are in the UK, please call 111 or Samaritans 116 123.
Summary
A psychiatrist in Fife #1 documents a serious incident of discrimination, that occurred whilst I was living in Fife. A psychiatrist, who had never met me or spoken to me – I didn’t know who he was – went into my medical records, and wrote a letter about me, which claimed that I have Factitious Disorder. He said that my facial pain is all made up ‘to feed the need to have a sick role.’ The psychiatrist sent this letter out to multiple agencies. The letter is now on my Scottish Medical and Social Work Records. This is an injustice that I will take to my grave.

My Hope
In the 50 years that I have been alive, there has been no mention of Factitious disorder anywhere on my medical records. The publication of this letter heavily influenced the way that I was viewed by the medical fraternity in Scotland. I am writing about this incredibly vulnerable incident because I want to raise awareness about the dangers of mental health discrimination within the system. I may never get justice for what has happened to me, but I am determined to prevent other vulnerable adults, from experiencing this level of assault and discrimination.

Context

In October, 2019, I fell into crisis. The impact of being knocked back by 13 NHS Trusts, on top of dealing with unrelenting facial and orbital pain for so many years, took its toll. The trigger to my breakdown, was the first incident that I wrote about in Medical Gaslighting #1 and a Head and Neck Unit in northwest England, who rejected my GP referral, with no reason provided. I want to avoid talking about my mental health at this point, to avoid conflating the physical and the mental. However, the impact that this ten-year fight to get treatment has had on my mental health has been profound.
Moving to Fife

I thought that if I crossed the border into Scotland, that I may get a better response from the medical services there, regarding my facial pain. In January, 2020, I left England and moved up to Fife. I arrived in Fife, in crisis. I was referred to the Mental Health Team, and I was admitted, under my request, onto a psychiatric ward for two weeks, to give me some respite. Following my discharge from the ward, I was assigned a Community Psychiatric Nurse (CPN). She phoned me on a weekly basis, to help me to manage my distress levels about my unresolved facial pain. I was not under the care of any psychiatrist.
The Scene

My GP in Fife referred me to an Ear, Nose and Throat (ENT) department, locally, regarding my facial pain. I saw an ENT Consultant at an NHS Hospital in November, 2020. He agreed to do an MRI scan of my parotid gland, and to then refer me to a Tertiary Head and Neck Unit. I went back to see this consultant after my scan. When I entered his consultation room, he had a face like thunder.
‘What’s wrong? I asked.
‘I have a letter here from your psychiatrist,’ he said. He had a menacing glare.
‘I don’t have a psychiatrist,’ I replied. Because, I didn’t.
He wheeled his chair forward, so that his face was close up to mine. ‘This psychiatrist says that you have Factitious Disorder, and that this is all fictionalization and somatization,’ he said, banging his pen on the desk.
‘Who is this man? I asked. ‘What is his name?’
The Consultant told me the psychiatrist’s name. I had never heard of this man. I genuinely did not know who he was. It was the consultant’s damning glare, that was so destabilising. This was a brutal attack on my integrity. It was a knife in the back from a stranger, akin to no other treachery.

What is Factitious Disorder?
Factitious Disorder is a serious mental disorder, in ‘which someone deceives others by appearing sick, by purposely getting sick or by self-injury. Factitious disorder symptoms can range from mild (slight exaggeration of symptoms) to severe (previously called Munchausen syndrome). The person may make up symptoms or even tamper with medical tests to convince others that treatment is needed.[1]

Doomed
My left ear pain was worsening. I was getting violent attacks of Pulsatile Tinnitus and my ear felt full. I was concerned, that I would not get a fair hearing about this, following the publication of this letter. The ENT consultant did still refer me to the Tertiary Head and Neck Unit, but he included this condemning psychiatrist’s letter, with his referral. This would undoubtedly affect the next consultant’s view of me. I stood no chance of getting any medical help now. My back was right up against the wall. My fists were in handcuffs.

This was mind-boggling. I had moved all the way up to Scotland, in search of medical help. Someone I had never even heard of had come up from behind, and shot me, for no reason. How could this happen? Was it even legal? I stood outside the hospital, trembling. I sent a text to my dear friend, Serena. Please call me, it’s urgent. I pressed send nine times.

The Psychiatrist

My friend came to see me that night. It was during the second national lockdown. We stood on my porch, two feet apart, both wearing facemasks. Serena told me that she had looked this psychiatrist up. He had only recently come out of an inquest, regarding the suicide of an eleven-year-old girl, who had hung herself, whilst under his care. I googled him. These are some of the links that I saw, online, about this psychiatrist.
Sophie and the Silent Experts (updated) – AntiDepAware
SHERIFFDOM OF SHERIFF COURT (scotcourts.gov.uk)
Inquiry hears Sophie, 13, could have been saved if system of support was in place (thecourier.co.uk)
The Inquest

The inquest into the girl’s suicide was damning. The Sheriff stated that if greater precautions had been taken, that the girl’s death could have been avoided. It was found that the system of care was confusing, the risk assessment and management was defective, recording of patient care was defective, and there was failure found to keep full records, particularly recording discussions between clinicians. The Sheriff found failure to categorise the girl’s suicide risk, lack of any formal diagnosis, and a lack of interaction with her school.

I couldn’t believe what I was reading. I looked at the dates. This psychiatrist had only come out of this inquest in August, 2020. He wrote this letter about me, in December, 2020, only five months later. I felt sick. Only five months after the inquest into his patient’s suicide, he started a position as a locum psychiatrist in Fife. He went into my medical records and he set off a lethal grenade.

The Citizens Commission on Human Rights
The Citizens Commission on Human Rights, (CCHR) is a non-profit mental health watchdog. It investigates abuse in the fields of psychiatry and psychology. It was co-founded in 1969, when people were still warehoused, abused and stripped of their rights. ‘Citizens Commission on Human Rights has long fought to restore basic inalienable human rights to the field of mental health, including, but not limited to, full informed consent regarding the medical legitimacy of psychiatric diagnosis.’[2]

I saw that The Citizen’s Commission on Human Rights’ website, listed this psychiatrist as one of the seven psychiatrists in the UK, responsible for the suicide of a patient.
Suicide While Under Psychiatric Care (cchr.org.uk)
I phoned them, and spoke with the director. He was very approachable, and confirmed that the CCHR knew of this psychiatrist. The director urged me to report this incident to The General Medical Council, (GMC) on the grounds of discrimination. He kindly offered to write me a letter of support. I don’t have faith in complaints procedures, particularly not with large regulatory bodies, but after I had seen the information about this psychiatrist online, I knew that I had a responsibility to act.
The Human Rights Act, 1998
‘The Human Rights Act 1998 sets out the fundamental rights and freedoms that everyone in the UK is entitled to.’
Equality and Human Rights Commission.
The scale of this injustice felt like an infringement of my human rights. I did not know who this psychiatrist was. How could he have therefore, written and published a letter on NHS letterheaded paper, stating that I have this serious mental disorder? I was in a state of deep distress and anxiety. I felt violated. The second organisation that I contacted was The Equality and Human Rights Commission, who signposted me to The Equality Advisory Support Service, (EASS). They provide non-legal advice to individuals who have experienced discrimination and breaches of their Human Rights. EASS thought that this letter, written and published by this psychiatrist, was a breach of two of my human rights.
My Human Rights

The two Articles from The Human Rights Act, that EASS thought this psychiatrist had breached were;
Article 8– Respect for Your Private Life, House and Correspondence. This includes the breach of my physical and psychological integrity, and the right to not be harmed.
Article 14– The protection from Discrimination. This means that you cannot be discriminated against on any status, which includes disability.
This psychiatrist had, without doubt, breached and undermined my integrity. It was a vicious attack, and a violent form of discrimination. He published this letter, so it was now available to view on my records. He also sent it out to multiple agencies. This made his action a potential breach of my human right to privacy.
I want this poisonous letter removed from my records. The Equality Advisory Support Service told me that I would need to go through the Human Rights Court to challenge it. The law dictates that you have one year and one day, from the incident, to take legal action. There was no way that I had the strength go to court; keeping myself alive was taking up all of my drive. I didn’t know what action I was going to take, but I knew that I had to act, not only to get justice for myself, but for those in the queue behind me. I would do whatever I could, to ensure that this unjust attack on my integrity would never happen again to anyone else.

Foot Notes
[1] Factitious disorder – Symptoms and causes – www.mayoclinic.org
Resources and Articles
People who have been affected by psychiatric abuse, are encouraged to contact the Citizens Commission on Human Rights and report what has happened. Reporting of psychiatric abuse and harm (cchr.org.uk)
Homepage | EHRC (equalityhumanrights.com)
The Human Rights Act | EHRC (equalityhumanrights.com)
Psychological Abuse: Types, Impact, and Coping Strategies (verywellmind.com)
Psychiatry, Abuses of | Encyclopedia.com

2023-10-23 11:26
Loose Cannon
Loose Cannon is an excerpt from my medical memoir. This is a work in progress. The genre is creative non fiction. It is based on real life events. All names have been changed to protect the identity of the individuals involved.
Chapter Three
November, 2013
Her name was Daisy. She had Crohn’s Disease. She was desperately thin, and she walked around the ward with a feeder tube in her nose. Daisy groaned and vomited through the night. By day, though, she went shopping, and returned to the ward with bags full of Adidas clothing. I admired her determination to carry on living her life. I envied her, not because I wanted a degenerative disease, but because she had a diagnosed condition, for which she received treatment. She was believed.

Professor Wong

Meet the Loose Cannon. I was under the care of The Clinical Lead of Ophthalmology, Professor Wong, at an NHS Teaching Hospital. Professor Wong specialised in ocular plastics, which is the medical and surgical treatment affecting the eyelids, the lacrimal, tear system, the bone around the eye, adjacent periocular (around the eyes), and the facial structures, including the forehead and cheeks.
He wore thin silver spectacles, and exerted a dictatorship style authority. From day one, our relationship was combative. My tone was exasperated. His was brusque. He started me on the oral antibiotic Doxycycline, for my orbital pain. He also took two blood tests. Both blood tests showed that I had raised neutrophils, a high white blood count, (WBC)and a raised Erythrocyte Sedimentation Rate (ESR). He wrote to my GP, and said that ‘the clinical evidence, points to infection as the cause,’ but he refused to acknowledge this to me.
IV Antibiotics

Professor Wong agreed to admit me on a for 48 hours of intravenous antibiotics. Once I was on the ward, I was contacted by a wonderful microbiologist. He was called Dr Penrose. ‘I will work with you for six months to find the right antibiotic,’ he said. He told me that he would administer Ciprofloxacin, intravenously, and that he would give me the strongest antibiotic that there is, for soft tissue infections, orally. This is the Super Daddy of antibiotics, called Linezolid. It penetrates muscle and soft tissue better than other antibiotics.

Over that weekend, kind-hearted nurses came and went to change my IV bag and to flush out my Cannula. I felt more energised from the treatment, but I still had the stabbing pain behind my eye and a swollen cheek. On the Sunday evening, I heard a kafuffle out on the corridor. The nurses were speaking to each other in hushed tones. I could hear them saying that Professor Wong wanted me gone by the end of the next day. I smelt trouble.
The Eclipsed Truth

It has always been difficult for me express myself truthfully to those in authority. I was raised by a middle-class family, who knew better than most, how to put on a show that ‘everything was fine,’ when in fact it was not. My mother was abusive toward me mentally and physically for most of my childhood and adolescence. She was also a secret alcoholic. No one knew that she drank. Not even me. It was at thirty years old, when I found a black binbag full of empty Whisky bottles under her bed, that I joined the dots, and realised that her weird behaviour was because of the alcohol.

My mother would hurl abuse at me most days, until I was so worn out, that I could not defend myself. After this, I would make her a cup of tea and tell that I loved her. I did that because I had no one else. I was frightened of losing her. That wasn’t the truth though. For the most part, I hated her, but my truth was eclipsed.
The Truth Gap

There was abuse from my father as well, but I did not realise that it had happened until I was in my early forties. That gap of thirty years between the trauma and the realisation that it had happened, means that when trauma or confrontation occurs now, I have a delayed reaction. I am unable to respond in the moment. I freeze, and then days or weeks later, I become furious. That is when I am able to say something, but by then, it is too late. The other person has moved on.

Keeping quiet is my default position. If I experience pain, I try to vocalise it, but my words get stuck. It is like my mind and my mouth are not connected. I know what I want to say, but when I speak, my words deflect and I become quiet and accommodating instead. My hope, is that the truth gap will lessen over time.

During child sexual abuse, the freeze response keeps us safe by keeping us still. It prevents something worse happening. It allows us to survive in the moment. But it manifests in the long-term as a learned helplessness, as an all-pervading sense of our powerlessness in our lives.
www.carolynspring.com
Angry Man

The sun shone through the sealed windows on the ward. I was sitting up in bed, eating a bowl of cornflakes, and I heard Professor Wong pacing up and down on the corridor.
‘I want her gone by the end of the day!’ he cursed.
‘Yes, Professor Wong,’ the ward sister replied.
I felt my throat constrict and my eyes prickle. He appeared, standing at the end of my bed. He was wearing a long raincoat, the kind you imagine a flasher, who is lurking in the bushes, would wear. ‘This is your last day of antibiotics,’ he said. ‘We will be discharging you today.’
‘But my face is still swollen, and my eye is still sore,’ I squealed.
‘My colleagues and I would like to speak with you.’ His eyes were stern. ‘We will see you in half an hour.’ He marched out of the ward, with his coat-tails flapping behind him.
Mr Andrews

Professor Wong reminded me of my headmaster at primary school, Mr Andrews. He would give the class a warning, before returning with the punishment. He once dropped a boy called Mark Sawyer onto his knees during an assembly, in front of the entire school, as a punishment for swearing. It was a wooden floor. We heard a thud, and then Mark’s long-drawn-out squeal. I thought of Mr Andrews when Professor Wong stormed off. I knew that he was coming back soon with my punishment. The ward sister agreed to accompany me to the meeting and Daisy took some photographs of my small eye and puffy face on my Blackberry.
‘Can you see my swollen face?’ I asked Daisy.
‘The left side of your face is completely different from your right side. Your face is lopsided,’ she replied.
The Meeting

It was a stuffy room. There was poor natural light, and horrible plastic chairs around the sides. The room smelt of cheesy feet and cold plaster. I was wearing my Snoopy pyjamas and trainers, and the cannula was still inserted into my vein. I laid my phone on the seat next to me, and sat with my hands pressed tightly under my bum. Professor Wong entered. Two consultants trailed behind him, both with short hair and grey suits. Professor Wong sat down next to me, reeking of boiled spinach.
‘You’ve had your 48 hours of antibiotics. My team and I have agreed that there is nothing more we can do for you here,’ he said.
‘But I feeling an improvement from the IV antibiotics,’ I pleaded. My voice was small. I could feel that familiar freeze within me setting in.
‘But the improvement is not significant enough to justify us continuing your treatment,’ he said. The scan was normal.’
I felt a jab in my heart. ‘But the blood tests showed infection.’ I looked up at the nurse for help, but she glanced down at the floor. ‘Look, Professor Wong. My eye is small and my cheek is swollen.’ I swiped the screen on my phone to show him the sequence of photos.
He flicked his hand at my face, like he was shooing away a stray cat. ‘I cannot see anything wrong,’ he said, pushing away my phone. ‘You are irrational.’
‘I am not irrational!’ I said. I dug to find force in my voice. ‘You don’t want to see that something is wrong. I am still in pain. Please do not stop my treatment, Professor Wong.’
‘There is nothing more we can do for you here. We’re done.’
Ouch!

The jab in my heart turned into a transforming sting. I looked up at the other two consultants. They looked like military officers on standby; quiet, but condescending in their poise. One of them was reading my notes, the other was looking down, with a pinched face.
My back was dripping wet. I could hear ringing in my ears. ‘The antibiotics are helping. The microbiologist said he would work with me for six months. Is that offer still open?’ I asked.
‘No, it isn’t,’ he replied.
That was it. The loose cannon was washing his hands of me.
The Fight

I refused to leave. I told the nurses that I wanted to see the Chief Executive, (CEO). There were phone calls back and forth from the ward to the CEO’s office. Later in the day, a nurse from the Chief Executive’s Office agreed to meet me in the main foyer. I ran down the stairs, still wearing my Snoopy Pyjamas, and carrying an Egg Mayonnaise sandwich in my hand. Families were milling around in the foyer. I found the nurse. She was podgy and wearing blue scrubs. She introduced herself as Rosie. We sat on the brown cushioned chairs, and I collapsed into her arms and fell into a paroxysm of weeping.
Rosie

‘Professor Wong is kicking me off the ward!’ I cried. ‘Can you help?’
‘I am aware, Felicia. I have little power. He is the consultant, and he has the last word.’
Rosie handed me a packet of tissues. I blew my nose. A lady with swollen ankles sat down next to us. Her husband was chomping on a Dime bar. I clung to Rosie, and nestled my head into her fat rolls around her tummy. ‘How can he just kick me off the ward, mid treatment?’
She said she would speak to him, but that she ‘could not promise anything.’ She got me a cup of cold water from the water machine. I drank the water, while my tears quietened.
Marching Orders

I got to stay one further night on the ward, after seeing Rosie. The next morning, Professor Wong marched into the ward, still wearing the same raincoat. ‘My colleague, Mr Sanders up at a nearby Hospital is willing to see you today,’ he said. His manner was milder, ‘but he is likely to say the same thing same as me.’
Professor Wong knew as well as I did, that his colleague would back up his opinion.
‘Who is he?’ I asked.
‘He was my mentor. He trained me,’ he replied. ‘We will send you up there in a taxi, but don’t expect a different opinion.’
‘OK, I’ll go and see him,’ I replied. I thought that something was better than nothing.
My Medication

My God! Then he really did shock me. He wasn’t just kicking me off the ward. He told me that he was stopping all of my medication as well. ‘I will be writing to your GP,’ he continued, ‘I will be advising that all antibiotics should be stopped after this final week’s course of oral Linezolid and Ciprofloxacin.’
A lump of tears rose in my throat. He wasn’t just kicking me off the ward. He was cutting my prescriptions dead without doing a blood test first. ‘But you haven’t done a blood test, to see if my infection markers are normal,’ I replied.
He squinted. ‘The medication that we give you will be your last lot.’ He started to walk away.
‘Professor Wong!’ I cried. ‘Please will you do a blood test, to check that everything is normal first?’
He ignored me and stormed off the ward.
Shock

I was winded. A lump of tears were stuck in my throat. He had admitted me for intravenous antibiotics, because of clinical evidence, that there was an infection in my system. He was now ordering that no further medication should be prescribed, without checking that my Neutrophil and White Blood Count were normal. Did he skip medical school when they taught about compassion? I looked up at Daisy, who was plaiting her hair.
‘Is he a doctor?’ Daisy asked.
‘Yep,’ I replied.
‘He doesn’t act like one,’ she said.
I was glad that Daisy saw the loose cannon for what he was. A nurse bought me my one week’s course of antibiotics in a stapled bag. While I waited for my taxi, Daisy came over and handed me a wooden doll. ‘This will bring you luck,’ she said and kissed me on the cheek. ‘Bye, Felicia.’
Two nurses escorted me down to the hospital entrance, where a taxi was waiting for me. I knew that this trip, to see the loose cannon’s colleague was a waste of time. Professor Wong was the most senior oculoplastic surgeon in the UK. If his clinical opinion was that I am irrational, then no other Ophthalmologist would contradict him.
‘Don’t worry, love. Everything always works out in the end,’ the taxi driver said. His name was Sunny.
The Taxi

As the taxi sped up the A64, I watched birds out of the window, spiralling in the sky. This was going from bad to worse. A collective opinion was forming around me, and about me, which was not positive. Something I once read at university came back to me. I took a course in my final year, called Comparative Epistemologies, which is the study of different knowledge systems. My tutor gave me a book called The Structure of Scientific Revolutions by Thomas Kuhn. Thomas Kuhn speaks about the emergence of paradigms and theories in science. He says that paradigms or theories emerge when there is enough agreement between people.

I gripped onto a bag of Skip crisps. Professor Wong was a medical consultant with enormous prestige. He had set in motion a theory that I was ‘irrational.’ If one or two more Consultants agreed with him, then a paradigm would emerge that I am irrational, and that there was nothing wrong with me. This theory would grow, and it would make getting a diagnosis and treatment impossible. I was slipping down a dangerous ravine, and there was nobody at the top to help me back up.

Recommended Articles

2023-10-19 01:34
Maxitrol
Maxitrol is an excerpt from my medical memoir, which is a work in progress. This is creative non fiction. It is based on real life events. All names have been changed to protect the identity of the individuals involved.
Chapter Two
Maxitrol
Maxitrol- it was the steroid eye drop, that set the flea bite alight. Trouble started as soon as I returned home from the monastery. I telephoned my GP, and told him that I had been bitten by a flea on my eyelid. He prescribed me a course of Cetirizine, which had no effect. The bump still nipped my eyelid. I later saw a Practice Nurse. She pulled down my eyelid with her finger, and said that my eyelid was infected. She prescribed me an antibiotic ointment, called Fusidic Acid. I asked her for an oral antibiotic, but she refused. I knew that the Fusidic Acid was not the right thing to give me, but the trust that we place in doctors, can pull us away from our instinct.

Fusidic Acid
I applied the acid drops to my eyelid. The Fusidic Acid stung. It made my eye water. What was a localised bump quickly morphed into swelling. My eye became puffy and my cheek was bulging like a balloon. I went to see my doctor. He diagnosed it as orbital cellulitis. He prescribed me Clarithromycin, an oral antibiotic, which is used to treat soft tissue infections. 
The Clarithromycin cleared up the swelling in my cheek, but it didn’t touch the stubborn bump on my eyelid . That gnarly bump still clinched to my eyelid. I started to panic. Growing up with a health-conscious mother, incidents concerning my health, as a young person, had been resolved with one visit to a doctor or to my local Accident and Emergency department. There was something stubborn about this. I didn’t like it. What had been a contained bump on my eyelid had now spread into some kind of infection. It was no longer a contained problem.

The doctors at my local practice had never dismissed me before, but, when I went back for the third time, the female doctor, spoke down to me. Your eye is fine. There is nothing wrong with your eye, Felicia.
Majorca
 I was due to go to Majorca for a holiday. Unsure whether travelling was wise, I flew out to sunny Palma with another two-week course of Clarithromycin. My orbital pain became stern. I paraded the promenade in Cala Millor. Not even the Bougainvillea or the sweeping views of the glistening Mediterranean could distract me from my worsening pain. I attempted every distraction, from perfecting my front crawl in the swimming pool, to taking day trips in a glass-bottom Catamaran along the Levante coast, where we passed dreamy bays and sea caves. Nothing worked.
I was due to go to Majorca for a holiday. Unsure whether travelling was wise, I flew out to sunny Palma with another two-week course of Clarithromycin. My orbital pain became stern. I paraded the promenade in Cala Millor. Not even the Bougainvillea or the sweeping views of the glistening Mediterranean could distract me from my worsening pain. I attempted every distraction, from perfecting my front crawl in the swimming pool, to taking day trips in a glass-bottom Catamaran along the Levante coast, where we passed dreamy bays and sea caves. Nothing worked.

I quietened my growing anxiety by smoking cheap packets of Marlboro Cigarettes and drinking Espresso’s in bars where old men played Draughts. In retrospect, I should have gone to see a doctor in Spain. My eyelid began to bulge, and my orbital pain developed into a stabbing pain behind my eye. I knew that this was an infection, because of my growing feeling of malaise. I was counting the days until my return flight headed home.
Accident And Emergency

As soon as the plane hit the runway at Manchester, I headed to an Accident and Emergency department, near where I lived. I sat in a plastic chair in the waiting area. I felt fatigued. An ophthalmologist with a petite frame and who wore chunky boots, and a chequered flannelled dress, called my name. Her brunette hair was tied back in pigtails. Her accent sounded Polish.
Blepharitis

The Ophthalmologist took me into a pokey room, with no windows. It was full with medical equipment. She put drops into my eye to enlarge my pupil. Once my pupils were enlarged, she looked into the back of my eye with her Ophthalmoscope. I rested my face on the narrow ledge, and felt her warm breath brush against my chin. She pulled down my lid with her finger, and diagnosed me with Blepharitis, which is inflammation of the eyelid. I told her that it felt like an infection, as the pain had moved to the back of my eye. She said that she did not want to give me antibiotics because of the harm they can do to my stomach. The no infection opinion started early on.
She prescribed me a two-week course of Maxitrol, which is a steroid eye drop, used to treat eye inflammation. I glanced down at the white and blue bottle. It said in bold writing that one Contraindication was Mycobacterial Ocular Infections. It is common knowledge that corticosteroids should not be used to treat active infections because they are known for their immune-suppressive effect and the long-term complications. I knew that these drops were the wrong thing to give me. I did not listen to my instinct.
Fire and Worms

I applied the Maxitrol eye drops into my eye twice daily, for one week. For a short while, my eye stopped hurting. It was after I finished the Maxitrol drops, that chaos ensued. It was a bright day. I remember it well. Sunlight was streaming into my South facing room. I suddenly felt my eyelid drop. Just like that. The left side of my face then went ablaze, like a wildfire had ignited and spread around the left side of my head.

It felt like there were hundreds of worms wriggling inside of my eyelid. Worse than that was, what felt like a sheet of mist, spread down my cheek, and around the left side of my head. My face became swollen. My eye was small, and my head felt heavy. It felt like I was wearing a helmet of bricks on my head. I knew that the Maxitrol Eyedrops were the wrong thing. That tiny localised bump under my eyelid was now a roaring inferno in my head.

Help!
The disaster that ensued from applying the Maxitrol eyedrops, just got worse. I ran from chemist to chemist, seeking help. No pharmacist could assist me. My orbital pain was insufferable. I still had that jabbing pain in the back of my eye. The flesh around my head was scalding hot. I knew that this was now a problem that I could not claw my way back from. There was no way back from this. There was something seriously wrong. I knew that I was in trouble.

Recommended Articles

2023-10-18 11:24
The Flea
The Flea is an excerpt from my medical memoir, which is a work in progress. This is creative non fiction. It is based on real life events. All names have been changed to protect the identity of all individuals involved.
Chapter 1
North Yorkshire
May 2013
The flea that bit me. It was a freak incident. I had booked a four-night stay at a Benedictine Monastery in North Yorkshire. The aim of the break was to give myself time out to grieve and rest, after the death of my late mother. I had once found refuge at a Franciscan Friary in Southern Indiana, USA. It was during a long hot summer, back in 2002, when I spent three months, writing my first book. It was when I was living and working in San Francisco as a dance teacher. I had taken a writing course in the vibrant Mission district. I had become spellbound by the power of writing.

The Friary
I had the summer months off from teaching. I sublet my room in the Lower Haight, and travelled by Greyhound Bus across America to stay at an Artist’s Colony near Kentucky, Indiana. It was a beautiful place, surrounded by acres of woodland and wildlife sanctuaries. I wrote in a sunny room by day, and when the sweltering heat mellowed, I spent the evenings, painting the fencing in the garden, to earn my keep. The Artist’s Colony was a place where writers stayed to work on projects, and it was situated on the grounds of the Friary. I had wonderful memories of sleeping in a plush bed with fluffy pillows, taking long walks through rolling woodlands where deer grazed, and having great chats with the Brothers and Fathers who dined with us at meal times.

A Retreat
2013– Life had not been kind. I was living back in England, rehabilitating from an injury. My mother, who I had had a complex relationship with, had recently passed away. I dreamed of my time in Kentucky, but I could not afford a Trans-Atlantic flight, so I sought out a similar place of sanctuary in England. I found a monastery in North Yorkshire. They offered room and board on a sliding scale for people on a reduced income, to come and enjoy the beautiful grounds and attend services if they wished. The rooms looked airy and clean in the brochure. No-where could replicate staying at The Franciscan Friary, but I hoped that I would find some tranquillity there.

The Monastery
The Monastery was situated on the outskirts of an affluent village in Ryedale. It was surrounded by sloping hills, and The Vale of Gilling was in the distance. It was home to a community of sixty monks who sought God according to the Rule of Benedict. The air was gentle and the gardens were awash with magnificent bluebells in full bloom, that spring afternoon, when my taxi pulled in to the grounds. I headed down to the Abbey to check in. It was a golden looking stone church with a huge steeple. I was greeted by a well-spoken woman, who explained that the reception was closing.

She walked me up a windy track to the residence where guests stayed, a stone’s throw from the Abbey. We passed a brown Hare eating grass shoots, but he dashed away through the trees as soon as he saw us. She led me into my bedroom. It was spacious and light and looked out onto orchards of apple trees. I could hear the bells from the Abbey, calling the monks for evening prayer. The woman wished me a pleasant stay and handed me the keys. My body slumped. I opened a window. A waft of medicinal scented breeze blew in. It was quiet, no human noise within earshot, only the chatter of birdsong and the brief rustle of wind.

The Bed
The double bed in the centre of the room was enticing. It had a brass head board and a bronze-coloured bedspread on top. My eyes were weighed down with grey bags. My body was so stiff, that it felt like I was carrying pockets of lead in my arms. I lay on the bed. The bedspread felt rough on my bare legs. I threw it off, and rested on the pink blankets instead. They were woollen blankets, the kind my mother used to store in the airing cupboard, and brought out once a year, when it was icy cold.
I closed my eyes and listened to the early evening tweet of the blackbirds. My stomach was rumbling, but I had missed the evening meal, so I pulled out a Whisper Bar from my rucksack and chewed on it, trying to make each bite last as long as I could. I felt ready for bed, so I slipped on my pyjamas, and tucked myself in under the sheet and blankets. I nestled into the bed, ready for a good night’s sleep.

Itchy Sheets
The sheets were scratchy. My skin began to itch. It did not feel like I was getting into a newly changed bed. The pillowcase smelt musky. It did not have that starchy feel and fresh aroma that linen has when it is new out of the laundry. I scratched my arms with my fingernails, and the backs of my calves with my feet, but nothing could satiate the itch.
The reception was closed for the night. There was nobody I could report the itchy sheets to. I considered sleeping on the bare mattress or should I sleep al fresco on the balcony? The thought crossed my mind, but catching a cold was a worse scenario than sleeping in an itchy bed. I closed my eyes, hoping that it would not be long until I would fall asleep. Little did I know, that what was about to happen was to change the course of my life indefinitely, and to throw me into a cyclone of ill-health and tragedy.

My Mother
I slowed my breath, and tried to feel the numbed emotion bubbling beneath my skin. My grief for my dead mother felt like a block of ice wedged between my breasts. The images of her just before she died were haunting. The memories of her lying in her hospital bed, emaciated, wearing a blue NHS gown, still made me shudder.
She had a hard bump around her stomach. It reminded me of the stomachs that the starving Ethiopians had during the famine in the 1980’s. The smell of my mum was heart-breaking. She had always been spotlessly clean. Growing up, her morning routine dominated our morning structure – her Radox filled bath bang on 7.00am, while her transistor radio blasted out LBC. Once dressed, she always smelt of Vitamin E cream and D’Issey Miyake perfume. That last day when I saw my mum. She was ill and gaunt and a stench of faeces wafted from her bed. She explained, that it was her stoma, that had been leaking.
Her Last Words
Her hair had not been washed for days. I asked the nurses to wash her hair, but I never found out if they did. I did not see my mother again. She was as spiky and restless as she had always been, but when I bent down to kiss her soft cheek, her final words were words that I clutched onto, like a child who clasps her beloved teddy that has lost most of its stuffing due to age.
‘You still smell the same…’ she croaked.
‘Smell the same as what, Mum? I don’t wear Chanel perfume anymore?’
‘No silly!’ she laughed. ‘You still smell exactly the same as when you were born.’

The hatred between us faded as fast as her life was ending. I wanted to calm the tremble in her voice, the day she arrived at the Marie Curie Hospice. I couldn’t. ‘Why am I here?’ she asked me on the phone. She sounded like a frightened child. ‘I thought I was going home…’
I had not seen my mother for the seven years before she died. That visit in hospital was the first and last time that I saw her. Due to her alcoholism and abusive behaviour, I had severed ties with my mum when I turned thirty years old. We had communicated since the severance, by letter only. The difficult decision to walk away from my mother was an act of self preservation and protection, but I knew that my decision had broken her heart.
‘Sorry for what I have done,’ I said.
‘I understand why you did it,’ she replied with a raspy voice. ‘Time would have passed anyway.’
That was enough. Her words echoed some kind of acceptance.
The Bite

It was around 9.00pm. I was still awake. My eyes were following the movement of the shadows, which were dancing on the walls. My flesh was itching. I looked down. I noticed three bites on my arms, and one on my stomach. They looked like flea bites. They were pink and inflamed. I thought about happier times to distract my attention away from the itchy bedding and my bites. I recalled wonderful days living on the Northern Californian coast, watching surfers cruise the waves on Ocean beach.
Out of the blue, something flew from my pillow. I think it was a flea. It bit me in my left eye. I felt a bump clinch my lower eyelid. I ran my finger along my eyelid, to make sure that there was nothing in my eye, but whatever it was that had bitten me and flown away. The lump felt gnarly. It was painful to blink. I tried to diffuse my anger. I had paid to come for a retreat to rest, but I was lying in a dirty bed, being bitten by fleas. This was not the respite that I had hoped for.
The Next Morning

The early morning sun, cutting through the thick orange curtain, woke me up at around 6.00am. The quiet was golden and the taste of chocolate from the night before repeated in my mouth. I could feel the bump, pinching my eyelid. There were more bites on my arms and my legs. I got a flashback to when I went backpacking around India with my boyfriend, when I was nineteen years old. After three months exploring Himachal Pradesh together, he went trekking in Ladakh for four weeks, while I travelled down to Goa and Karnataka with a friend.
We had agreed to meet up four weeks later outside McDonalds in Connaught Place, Delhi. En-route to meet him in Delhi, I stayed overnight in a hostel in Bombay. I slept on a top bunk in a dormitory, and had made sure to sleep on top of my rolling mat. Woken to the sound of Chaiwallahs the next morning, I was covered from head to toe in red bites. I had been eaten alive by bed bugs in the night. Our first night back together in Delhi, my boyfriend and I stayed in a hotel in Paharganj, where he poured soothing trickles of Calamine lotion over my sore skin before making love to me. We travelled onwards to Rajasthan. I was plastered in that pink lotion for weeks, scratching my way around the colourful continent.

The Chambermaids
I studied my face in the mirror. My eyelid was red and sagging. My body felt sore. I questioned whether I should leave for home or stay, and see a doctor when I got home. A little while later, I heard muffled waves of female camaraderie and laughter coming through my wall. I put on some clothes and went out to see who it was. Next to my bedroom was a common room, the type you find in university halls of residences. It smelt of faded disinfectant and powdered chicken soup. Sitting around a table, drinking tea, were three chambermaids. They wore blue short-sleeved aertex shirts and matching hair nets. They looked up in unison when I walked in. A look of disapproval shot across their faces, like I had interrupted something important.
‘The sheets…’ I said. ‘They are not clean. Please can you change them immediately, I have been bitten.’
I held out my arms to show them the flea bites. Their heads turned to one another. ‘I’m sure that the sheets were changed,’ one of the ladies said, gazing up at me. Her voice was faint. ‘But we’ll change them for you this morning if you want.’
‘Do you always change the bedding when a guest leaves?’ I asked. They had gone back to dunking their Digestive biscuits in their tea. I felt my cheeks redden. I raised my voice. ‘Do you always change the bedding?’ I repeated.
‘Yes, of course we do,’ one of them, replied, looking at me momentarily, and then dipping her head back down.
‘Well, I think you missed my bed,’ I snapped, before going back into my bedroom and slamming the door shut behind me.
I heard no more laughter. Only the sound of scraping chairs, and then they scuttled.
Breakfast

I headed down to the Abbey for my breakfast. The sky was belting blue. Sheep grazed in the distant fields, and Bumblebees hovered around the flower beds. The lady who had greeted me the evening before, was typing at her desk when I walked into reception. She was wearing a red dress and her hair was pushed back with a diamante headband.
‘Is everything OK with your room?’ she asked politely.
‘The bed is not clean. I have been bitten by fleas.’ I pulled up my sleeve and showed her my bitten arm.
The lady gulped. She picked up the phone, and punched in the digits with her finger. Change the sheets immediately, I heard her say in a grave tone. After a fry up, toast, and a pot of tea, I returned to my room to find an army of cleaners, stripping the bed and cleaning the room, using dusters and spray liquids. My room smelt of citrus fruits. The sheets were stiff and smelt of lemons. I decided to spend the remaining three days at the monastery, but it was not a happy stay. My body was in pain. My flea-bitten flesh was inflamed and sore.
It is difficult to believe that a flea bite to my eyelid could unfold into a decade-long tragedy. But it did.
The flea that bit me. This is how my facial pain began.

A boy with swollen eye from insect bite.
Recommended Articles
The Aesthetic Memoir- Interview with Damian Barr
Interviews with Natalie Goldberg

2023-09-29 11:06
Is This Lyme Disease?
Summary
Is This Lyme Disease? asks whether my persistent infection of ten years could be Lyme Disease. Lyme disease is a tick-borne bacterial infection that is caused by the bacteria Borrelia Burgdorferi. It is also known as borreliosis, and it is spread through the bite of an infected tick. The early signs and symptoms of Lyme disease are a circular or oval-shaped rash around where the tick-bite occurred.

A Cool Dentist
I had a wonderful dentist in Halifax, West Yorkshire. She would belt out pitchy renditions of Beautiful South songs while she doing a scale and polish. I can remember so clearly how convinced she was that I had Lyme disease. It was the chronicity of my symptoms that fuelled her conviction.

My singing dentist urged me to contact the Phones 4U founder, John Caudwell. John Cauldwell hit the UK headlines in 2018, when he and his family were struck down with Lyme Disease. He pledged his own money in a bid to spark a government-led research program into Lyme disease ‘to improve the NHS’ woeful lack of understanding of the illness.’ [1] Five years on, I question whether my dentist may have been right. Do I have Lyme disease?
How It Started

My illness began in 2013. It started with a flea bite. I think it was a flea that bit me, but I’m not entirely sure. I was staying at a monastery on a residential retreat. This monastery was in North Yorkshire. It was surrounded by rural woodland, where there are relevant tick and wildlife populations.

The chambermaids had not changed the bed sheets in my room before I arrived. I stupidly got into the bed. Fleas bit me on my arms, legs, and stomach. One flea bit me on my left eyelid. Immediately, I had a red bump on my eyelid. That bump clenched my eyelid for five months. The red lump didn’t resemble the classic oval Lyme rash, but because it was on my eyelid, perhaps it looked different. My infection stemmed from that red bump. The swelling spread from my eyelid, down to my cheek, and around the left side of my head.
Lyme Symptoms – Stage 1
There are three stages to Lyme disease symptoms. Stage 1 is the Early Localised Stage. Symptoms include fever, headache, fatigue/loss of energy, malaise, chills, neck pain, muscle aches, and swollen lymph nodes. I can remember the early stage of my illness vividly. I suffered all of the symptoms associated with the first stage of Lyme. During the first two years, I had no energy. I had constant chills, especially around my parotid area, and I was exhausted. I suffered with muscle aches and a very stiff neck. For the entire 11 years, I have had a consistently raised neutrophil and white blood count, indicative of bacterial infection.

Lyme Symptoms- Stage 2 & 3
I suffered with the symptoms that are congruent with stage 2 of Lyme disease. This is known as the Early Disseminated Stage. My symptoms were neck pain, an irregular heartbeat (tachycardia), painful swelling in the tissues of my eyelid and eye, swollen lymph nodes, and flu-like symptoms. I have not suffered with pain or numbness in my hands or feet. Nor have I had joint pain. I have not experienced arthritis in my joints either. Arthritis is a symptom that is associated with the late-disseminated stage. However, according to The Mayo Clinic, in the late stage, ‘you may still have symptoms from the earlier stages, and more serious cases may also cause damage to tissues.’ [2]
Reflection

What the Mayo Clinic says about patients experiencing early-stage symptoms later on resonates with my experience. I still have painful swelling in the tissue around my left eye. Doctors detected reactive lymph nodes in my soft tissue. If I do not take antibiotics, I become unwell and weak. It seems possible from looking at my radiology images that the soft tissue on the left side of my face is calcified. I haven’t been able to find out about this. Medical consultants have been unwilling to answer my questions, but I do wonder if this could be Lyme-related.
Doxycycline

Doxycycline is an antibiotic from the tetracycline class. It treats a broad spectrum of bacterial infections, including urinary tract infections, respiratory, ophthalmic, and soft tissue infections, cellulitis, and erysipelas. It is a first-line standard of treatment for adults with Lyme disease. Doxycycline treats all aspects of Lyme, including Lyme arthritis and Lyme carditis.
It is currently one of the antibiotics recommended for the treatment of Lyme Disease by the Infectious Diseases Society of America.
Medical News Today.
According to The UK’s National Institute for Health and Care Excellence (NICE), other antibiotics, which are effective treatment options for Lyme disease are; Azithromycin, Ceftriaxone, Cefotaxime, and Amoxicillin. In On Antibiotics, I explain that Doxycycline and Cefalexin are two of the most effective antibiotics for my facial pain, (aside from Linezolid). Doxycycline has been a mainstay medication for me over the last ten years. It subdues my symptoms, my energy levels increase, and I feel much better systemically, when I take it, but when I come off these tablets, my symptoms return.

Cephalexin is also a highly effective antibiotic for my facial pain. It soothes the localised symptoms most effectively, but it does not give me the same relief from the systemic feeling of malaise that Doxycycline provides. Cephalexin is from the same Cephalosporin family as both Ceftriaxone and Cefotaxime. These antibiotics are also effective standards of treatment for Lyme disease.
Reflection

Doxycycline and cephalexin are the most therapeutic antibiotics for my condition. They subdue my symptoms faster and more effectively than other medicines. They are both first-line standards of treatment for Lyme disease. Therefore, I wonder if it could be the latent Borrelia Burgdorferi bacteria in my system, or soft tissue, that is responding to these antibiotics.
Lyme Testing

The website IGeneX.com, explains that the most accurate Lyme tests are serological tests. ‘They do not detect the bacteria or its antigens, but they detect the antibodies, that an infected person produces in response to these antigens.’[3]
The most common Lyme Disease tests are, Enzyme-Linked Immunosorbent Assay (ELISA) and the Western Blot. Both show the reaction between antibodies in an infected person’s blood to the bacteria, causing Lyme Disease. To receive a diagnosis of Lyme disease, you must test positive with both Elisa and Western Blot blood tests. According to IGeneX.com, there are numerous strains of Lyme Borrelia. The Elisa and Western Blot tests can only detect one strain. These tests, therefore miss infections caused by other strains. IGeneX.com has created its own Immunoblot Lyme test to solve these problems. It is a ‘serological test, that increases specificity, so that more species of Lyme Borrelia are detected.’ [4]

A common problem with Lyme disease testing is that antibodies do not show up early on in the disease. If a patient tests too early, his/her body may not have produced enough antibodies to show up in a test. This can create a false-negative test. I had two Lyme disease tests in 2014. Both of my Lyme serums came back negative, but I had both of my Lyme disease tests done within the first three months of my illness. I do not know which Lyme disease tests the clinician used. However, if antibodies for Lyme disease do not show early on, I wonder if my Lyme test results could have been false negative ones.
If your blood test comes back negative, that does not necessarily mean you don’t have Lyme Disease.
Global Lyme Alliance
Chronicity of Symptoms

An infection lasting eleven years is extraordinary. It is possible that I have suffered with an infection for eleven years. I have been reading material about persistent symptoms in Lyme Disease, published by The John Hopkins Lyme Disease Research Centre.
The information available through this research centre explains that untreated Lyme disease will become a chronic, persistent infection in the majority of people. It says that people who develop chronic symptoms can be related both to the bacteria Burgdorferi and to the human immune response to the bacteria. Additionally, an infection may start in the skin at the site of the tick-bite but then enter the bloodstream and the lymphatic system. It can then affect certain tissues, including the neurological system. Delayed diagnosis can be a contributing factor in persistent symptoms, and Lyme disease can be complicated by other infections. If somebody gets more than one infection from a tick-bite, it can create a more complicated infection.
Rigorous evaluation is necessary to determine if Lyme disease could be the trigger for ongoing disease processes.
John Hopkins Lyme Disease Research Centre.
Post Treatment Lyme Disease
The John Hopkins Research Centre explains that Post-Training Lyme Disease (PTLD) is the term used to describe people who go on to have ongoing symptoms despite receiving treatment. The John Hopkins Centre states that the mechanisms behind PTLD could be autoimmunity and immune dysfunction, inflammation due to persistent bacteria, or left-over bacteria that have not been eradicated during treatment. Auto-immunity and immune dysfunction can also cause inflammation.
Final Reflections

Doxycycline and cephalexin are the two first-line treatment options for Lyme disease, both of which I respond positively to. I have suffered with the symptoms that are synonymous with the first 2 stages of Lyme disease. I have had raised infection markers for 11 years, particularly my neutrophils. This indicates the presence of a bacterial infection. It is so frustrating that the surgeon who removed my parotid tissue in 2018 did not culture it. If he had done so, we may have found out what this was. However, we still do not know what the bacteria is that is potentially causing my facial pain. I do wonder if the bacteria, Borrelia Burgdorferi is causing my illness. Or, if I have had Lyme disease, which has developed into a chronic infection?
The article What to Know About Doxycycline for Lyme Disease in Medical News Today, states that ‘due to Doxycycline being highly protein-bound in circulation, it is unlikely to sufficiently diffuse into the tissues affected by Lyme disease bacteria.’ I am curious if this could explain why the repeated doses of Doxycycline that I have taken over the years, has not penetrated my soft tissue sufficiently.
Was My Dentist Right?

Was my singing dentist right? Do I have chronic inflammation that is caused by bacteria that has not been eradicated? Have I got an immune dysfunction? Is my illness Lyme Disease, or a chronic infection that untreated Lyme Disease triggered?

I am seeking a physician or infectious diseases consultant who can diagnose and treat my chronic symptoms of eleven years, which seem most congruent with bacterial infection. If you are a physician with an interest in chronic infections and Lyme disease, please get in touch. You can email me at info@myfacialpain.com, find me on X @myfacialpain, or message me via the contact form on my website. Thank you.

References
[1] Caudwell, John; I have taken these words directly from the letter that John Caudwell wrote to the then, Health Secretary, Jeremy Hunt, in 2018.
[2] Mayo Clinic; Lyme Disease; Symptoms and Causes.
[3] IGeneX Inc; The Best Test for Lyme Disease
[4] IGeneX Inc; The Best Test for Lyme Disease
Recommended Articles
Lyme Disease Diagnostic Research
Recommended Videos

2023-09-18 06:56
No To Botulinum Toxin
Summary
No to Botulinum Toxin discusses the reasons why I have refused Botox injections for my facial pain. Botulinum Toxin (BTX) is a strong bacterial toxin, created from fermentation of clostridium botulinum. It is ‘a neuromuscular blocking agent that triggers chemical denervation by temporarily suppressing secretion of acetylcholine at major nerve endings; therefore, Botox injections are useful for diseases with increased muscle activity or tension.’ [1]

Facial Pain Disorders
Botulinum Toxin is used in the treatment of many facial pain disorders by producing temporary skeletal muscle relaxation. In Pain Management, Botulinum Toxin has an ‘analgesic effect by reducing muscle hyperactivity.’ [2] I have been offered Botox injections to manage my facial pain, but I have refused the offer of these injections. I will explain my reasons for refusing BTX injections later on the post. Firstly, the following facial pain disorders that are managed with Botox (BTX) injections include;
Oro-Facial Pain

BTX is very effective for the management of Muscular Temporomandibular Joint Disorders (TMD) and hyperactivity of masticatory muscles. Symptoms of TMD include; pain around the jaw, popping and clicking noises when you move your jaw, difficulty opening your mouth, and jaw lock, when you try and open your mouth.
Trigeminal Neuralgia.
Botulinum Toxin A injections are a safe and effective method of management of Trigeminal Neuralgia. ‘Trigeminal Neuralgia (TN) is a painful disorder, which presents as recurrent, unilateral, brief but severe, electric-shock-like pains of rapid onset and duration. It normally remains within Trigeminal dermatomes.’ [3]
Myofascial Pain Syndrome

Myofascial Pain Syndrome (MPS) is a regional pain syndrome, which is characterised by painful points (trigger points) in the masticatory muscle system. Symptoms include pain in the muscle, muscle knots and muscle spasms. ‘Botulinum Toxin blocks the communication between nerves and muscles, and inhibits muscle contractions in the muscles where the painful points are located. This may result in pain relief when injected into the area.’ [4] In summary, Botulinum Toxin helps with both Myofascial Pain Syndrome and TMD. It can be injected into Head and Neck muscles to relax muscle function and spasm.
Salivary Gland Application
Ultrasound-guided Botulinum Toxin injections are used to treat Sialorrhea, which is excessive salivation or drooling. An injection of Botox into the salivary gland reduces the production of saliva, and thereby the frequency of the patient’s drooling. Patients can develop chewing problems and swallowing difficulties as a side effect from these injections. Sialadenitis is chronic inflammation and swelling of the parotid gland. It is usually caused by obstruction, or a ductal thinning (stenosis.) Botulinum Toxin injections into the parotid gland are known to be effective in temporarily reducing pain and swelling associated with Sialadenitis.
Refusal of Botox

I have been offered BTX injections for my facial pain. The reason that I have refused them is because I do not suffer with any of the above conditions. I have not received any diagnosis, so we do not know what we are treating or dealing with. I do not suffer with Trigeminal Neuralgia, (TN). My symptoms are not congruent with TN. I have no symptoms related to jaw pain or disorder, and the symptoms related to Myofascial Pain Syndrome are not congruent with mine. If I had been diagnosed with any of these disorders, then I would be open to accepting BTX injections, but I have not.
Parotid Gland and Masseter Muscle

I do have a major problem with my left salivary gland, but it is not excessive salivary production or drooling, (Sialorrhea) that I suffer with. The malfunction in my gland has been detected as a thickening of saliva, a thinned duct, hardened tissue and reactive lymph nodes. The parenchyma was Sialolithiasis. I understand that Botox injections slow down the production of saliva, so these injections may temporarily stop the gland swelling, but that would be empirical symptom management, not definitive treatment or long-term cure. After suffering for ten years, and having tried temporary wash outs, I do not wish to return to short term ‘management.’ Additionally, if infection is the underlying cause for my parotid gland disease, then BTX could create further problems.
I understand that Botox injections relax muscle function and spasm, but I do not suffer with overactive masticatory muscles. My left masseter muscle is enlarged, not overactive, and my muscle pain is closely linked to the problem with my parotid gland. A scan done one year after my surgery, showed that there is accessory parotid tissue over the masseter muscle. I have asked many consultants, if the pain in my masseter muscle could be caused by the ongoing problems in my parotid gland. I have received no answer.
Cure Not Management

Radiology image 1

Radiology Image 2

Radiology Image 3
Botulinum Toxin injections are effective pain management for some facial pain syndromes. However, BTX is a temporary suppressant, not a definitive cure. It is common for pain to return three to six months after the injection. Abnormality has been detected in the soft tissue and muscle in my left cheek, and around my left eye. That abnormality needs diagnosing and treating, not suppressing with ‘symptom management.’
Facial pain syndromes can be very heterogeneous and need individual diagnosis and treatment.
Head and Face Medicine, BioMedCentral.com
Finding A Cause

I clarify in This is Not Chronic Pain, the difference between pain conditions that need ‘managing,’ and pain conditions where there is an aetiology, (cause) and which need treatment. My facial pain is not chronic pain, which just needs managing. I have ‘managed’ my facial pain with oral antibiotics for ten years. The pathology thus far found, pushes for the need to identify a cause for my facial pain, so that I can receive the correct treatment.
My left-sided facial pain involves a left diseased parotid gland, severe periocular pain, left ear pain, and left-sided head pain. Pathology found includes a collapsed levitator on my eyelid (left ptosis), parenchymal damage in my parotid gland, reactive lymph nodes, masseter enlargement and buccal fat pad abnormality. There have also been consistent raises with my white blood count, particularly my neutrophils.
Diagnose Me First

Infection is the suspected aetiology for my facial pain. Botulinum Toxin is not a recommended treatment for soft tissue infections. If I am suffering with a soft tissue infection, Botulinum Toxin could make my symptoms worse. It is imperative, therefore that I receive a diagnosis before injecting Botox Willy-nilly into my face. It is not clear what we are treating. I do not, therefore, want a dangerous chemical injected into my face, without receiving a diagnosis first.
Botulism

I will also not accept Botox injections because of the significant risk of Botulism. Botulism is when the toxin, Clostridium Botulinum, attacks the muscles. This can result in a serious bacterial infection, that can cause life-threatening illness. The symptoms of Botulism begin in the muscles and eyes of the face. They include, drooping eyelid (ptosis), loss of facial expression, drooling, reduced gag reflex and breathing difficulty. I already have a drooping eyelid, (left ptosis) as part of my condition, and I suffered with severe loss of facial expression, following my superficial parotidectomy in 2018. I am not, therefore, opening myself up to the risk of Botulism, on top of what I am already suffering with. No way.


‘Facial pain, alone or combined with other symptoms, is a symptom situated at a cross point where several disciplines meet; Ophthalmologists, Ear-Nose-Throat, internal medicine and neurosurgeons. Key message: Caregivers should “think outside of the box” and refer to other disciplines when indicated. If not, a correct diagnosis can be delayed and unnecessary treatments might be given.’
Facial Pain- A Review and Proposal for a Pragmatic Diagnostic Approach- Research Gate
References
[1] Lew, MF; Review of FDA- Approaches of Botulinum Toxins, including Data Efficacy in Pain Reduction, National Library of Medicine, PubMed, November, 2022
[2] Woo, SS; Application of Botulinum Toxin in Pain Management, National Library of Medicine, PubMed Central, March, 2011
[3] Rubis A; The Use of Botulinum Toxin A in the Management of Trigeminal Neuralgia; A Systemic Literature Review. Journal of Oral & Maxillo Facial Research (JOMR), April, 2020
[4] Atallah A and Silva EMK; Botulinum Toxin for Myofascial Pain Syndrome in Adults, Cochrane Library, National Library of Medicine, PubMed Central, July, 2014
Recommended Articles
Facial Pain: A Comprehensive Review
Botulinum Toxin in Pain Management
Botulinum Toxin For Pain Relief?
Myofascial Pain Disorder- An Overview.
Botulism: Types, Causes, Symptoms and Treatments
Ultrasound-Guided Botulinum Toxin Injections for the Treatment of Drooling
Improvement of Chronic Facial Pain with the Help of Botulinum Toxin

2023-09-06 07:27
On Lymphoedema
What is Lymphoedema?
Lymphoedema is a long-term chronic condition. It ‘refers to tissue swelling, that is caused by a build-up of lymph fluid, that is usually drained through the body’s lymphatic system. Lymph nodes are a vital part of the lymphatic system. Any type of problem that blocks the drainage of lymph fluid can cause Lymphoedema.’[1]

Symptoms
The symptoms for lymphoedema include; swelling, a feeling of heaviness or tightness, repeated skin infections and tight or thickened skin. Fluid leaking through skin or wart like growths, are also symptomatic of lymphedema. Many of my symptoms are congruent with those of lymphoedema. I have persistent swelling on the left side of my face. The tissue feels tight and heavy, and I have had recurrent infections in my parotid gland for many years. Hardened, calcified tissue was found in my parotid tissue, as were reactive lymph nodes. I do not have fluid leaking through the skin.

‘Lymph nodes play a vital role in protecting the body against infection and disease. They contain immune cells that detect and destroy bacteria.’
Medical news today.
Function of Lymph nodes
The lymphatic system is a network of lymph glands and vessels that help fight infection and remove excess fluid. The function of the lymph nodes is to drain fluid, filter out harmful substances, and fight infection.
Human Lymph Nodes Anatomy Illustration
Tissues in the body excrete lymphatic fluid or lymph, in order to eliminate waste products. The vessels take excess fluid from the body’s tissues and direct it towards the lymph nodes. The lymph nodes then filter lymph fluid and destroy the bacteria, as it arrives from the scalp, neck and face. They then release the clean fluid back to the blood. A lymph node swells when it has to work hard to remove harmful substances from the lymph fluid. Lymphadenopathy is when lymph nodes swell, and this swelling is normally caused by either cancer or infection.
The Lymphatic system, acts to drain fluid from the tissues and return it to the circulation.
Teach Me Anatomy.
The Facial Lymphatic System
‘There are around 800 lymph nodes in the human body, and approximately 300 of these, are in the head and neck region. Henri Rouvière was the first to classify cervical lymph nodes in 1932 into; Submental, facial, submandibular, parotid, mastoid, occipital and retropharyngeal node groups.’[2]
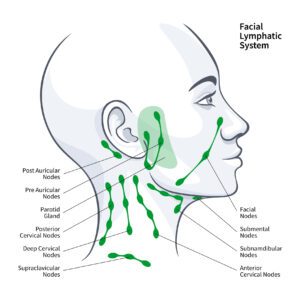
Head and Neck Nodes
- Occipital: These lymph nodes are located in the back of the head. They collect lymph from the occipital area of the scalp.
- Mastoid: There are 2 mastoid lymph nodes, called the post-auricular lymph nodes. They are located posterior to the ear and lie on the insertion of the sternocleidomastoid muscle into the mastoid process. They collect lymph from the posterior neck, upper ear and the back of the ear canal.
- Pre-auricular: Pre-auricular lymph nodes are located anterior to the auricle of the ear, and collect lymph from the superficial areas of the face and temporal region.
- Parotid: The parotid lymph nodes are a small group of nodes located superficially to the parotid gland. They collect lymph from the nose, the nasal cavity, the external acoustic meatus, the tympanic cavity and the lateral borders of the orbit. There are also parotid lymph nodes deep to the parotid gland that drain the nasal cavities and the nasopharynx.
- Submental: These lymph nodes are located superficially to the mylohoid muscle. They collect lymph from the central lower lip, the floor of the mouth and the apex of the tongue.
- Submandibular: Three to six nodes are located below the mandible in the submandibular triangle and collect lymph from the cheeks, the lateral aspects of the nose, upper lip, lateral parts of the lower lip, gums and the anterior tongue. They also receive lymph from the submental and facial lymph nodes.
- Facial: This group comprises the maxillary/infraorbital, buccinator and supramandibular lymph nodes. They collect lymph from the mucous membranes of the nose and cheek, eyelids and conjunctiva.
- Superficial Cervical: The anterior nodes collect lymph from the superficial surfaces of the anterior neck. The posterior lateral nodes collect lymph from superficial surfaces of the neck.’[3]
A Clever Rheumatologist

I consulted with a clever rheumatologist about my facial pain, at a private hospital in London from May, 2014- February, 2016. He was the consultant, who I have seen the most consistently during this ten-year episode, and who I trusted. The rheumatologist was unable to give me a definitive diagnosis, so he treated my condition with empirical therapy. He examined the consistent raises in my neutrophil count, White Blood Count and ESR, and saw first-hand how oral antibiotics stabilised my bloods, and how much better I was when I took them. He prescribed long-term antibiotics, which significantly stabilised my condition.
Empirical Treatment

The antibiotics that the rheumatologist prescribed cyclically were; Rifampicin,600mg, Doxycycline, 100mg, and Cephalexin, 500mg. We tried Levofloxacin and Ciprofloxacin, which we had to stop, because I developed Achilles Tendonitis as a side effect from taking them. We also tried Clindamycin, 500mg, Metronidazole, 400mg and Azithromycin, 500mg. These antibiotics (apart from Rifampicin,) are all known to treat complicated soft-tissue infections. They controlled my symptoms, but when I stopped taking them, my infection markers shot up, and my symptoms returned.
Lymphatic Drainage Damage
The rheumatologist thought that my facial pain and swelling was possibly caused by lymphatic drainage damage, and that I could be suffering with Lymphoedema. He thought that the infection had damaged the lymphatic drainage on the left side of my face. This meant that lymph fluid was not draining away, and infection was not being killed off. He thought that lymphoedema could explain the stubborn nature of my facial pain and swelling, and why my symptoms returned when I stopped taking the antibiotics.
The Parotid Gland
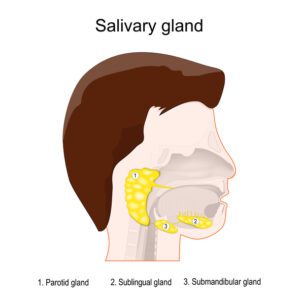
Human’s head with three main paired salivary glands: Parotid, Submandibular, and Sublingual. Exocrine glands that produce saliva through a system of ducts.
The parotid gland has been the main source of my facial pain. In 2015, the pain in my masseter and parotid region was so bad, that I was unable to eat or drink. The rheumatologist identified that the problem was my left parotid gland. He referred me to Oral Maxillofacial surgery. It was detected, via ultrasound scanning and sialography that there was obstruction and a thickening of saliva in my left parotid gland, which was treated with ongoing sialendoscopies.
Parotid Gland Histology

In 2018, I had some of the superficial lobe of my parotid gland removed. The histology showed; dense secretions in the ducts, hardened tissue, and reactive lymph nodes. The parenchyma was sialolithiasis. A scan done, one year after surgery showed that there is still some superficial lobe remaining, the deep lobe is all there, and there is some accessory parotid tissue over the masseter muscle. The residual tissue is rock hard. It swells when I eat and drink, causing the left side of my face to inflate.
My Facial Pain
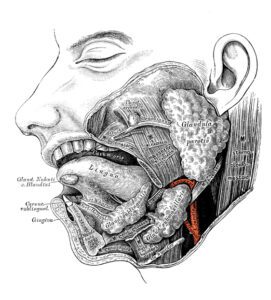
In My Facial Pain, I explain that whilst the main source of pain is in the masseter and parotid region, I also have pain in the middle of the cheek, which extends all the way up to my zygomatic arch. Alongside the pathology found in my parotid gland, left masseter enlargement has been identified, and benign abnormality has recently been detected in the buccinator, maxillary region.

An MRI Neck radiology image, showing unexplained abnormality in the left buccinator, maxillary region.
A radiology image from an MRI Neck scan, showing unexplained abnormality in the left buccinator, maxillary region.
A radiology image from an MRI Neck scan, showing unexplained abnormality in the left buccinator, maxillary region.
The facial lymph nodes, which reside in the maxillary, buccinator region, collect lymph from the nose and cheek. The submandibular nodes also collect lymph from the cheek. The pre-Auricular nodes, which sit within the parotid gland, just in front of the ear, collect lymph fluid from the superficial areas of the face and temporal region.
Question
If I do have lymphedema, and if my lymph nodes are not draining fluid away, could this explain the persistent pain and swelling in the superficial and temporal area of my face?
My Periocular Pain

In My Periocular Pain, I describe the pain and swelling around my left temporal artery and upper eyelid. The lymph nodes within the parotid gland, which, in my case, have been found to be reactive, collect lymph from the lateral border of the orbit. The facial nodes, which reside in the maxillary, buccinator region also collect lymph from the eyelids. As abnormality has recently been detected in the buccinator and maxillary region, I am wondering whether these lymph nodes could be damaged.
Question
Is it possible that my persistent periocular pain and swelling is being caused by the facial and parotid gland lymph nodes not draining away fluid from my eyelid?

MRI Neck scan image, showing unexplained left periocular swelling.
My Ear Pain

In My Ear Pain, I explain that my symptoms include a feeling of pressure and fullness in my left ear. This is not dissimilar to Airplane ear (ear barotrauma), which people experience when on an airplane that’s climbing after take-off, or descending for landing. I asked was whether my left ear pain was being caused by Eustachian Tube Dysfunction, or the enlarged mastoid on the affected side.

A radiology image from my CT Neck scan, from 2021. It shows an enlarged mastoid on the affected, (left) side.
Question
Further research that I have done into the facial lymphatic system has raised new questions. The lymph nodes, within the parotid gland, collect lymph from the acoustic meatus (the ear canal). The Post Auricular/mastoid nodes, behind the ear, where I experience pain, collect lymph from the upper ear and the back of the ear canal. If I am suffering with lymphedema, could my left-sided ear pain be an accumulation of lymph fluid that the parotid and mastoid lymph nodes, are not draining away?
Reflections

One of the things that has baffled so many physicians, is that ten years is an unusual amount of time for a soft tissue infection to go on for. It is unclear why the oral antibiotics that I take do not clear it away. If the lymphatic drainage on the left side of my face is not functioning properly, the lymph nodes will not be able to fight off infection. They will neither be able to drain away excess fluid. This may explain a) the stubborn nature of this infection, b) my persistent facial swelling and c) why the oral antibiotics only partially work.
I am unsure if lymphoedema explains all of my symptoms. However, I do wonder if it could be a contributing factor behind my facial pain. The question is; with a delayed diagnosis and treatment plan of ten years, is it too late for this to now be treated?

MRI Neck Radiology image, showing difference on affected (left) side.

MRI Neck radiology image, showing abnormality in left cheek and eye.

Radiology image, showing abnormality in left parotid region.

Footnotes
[1]Lymphedema – Symptoms and causes – Mayo Clinic
[2] Dr Moideen, SP; Lymph Node Levels of Head and Neck, DrSamu.com
[3] Fitzgerald, G; Lymphatic Drainage of The Head and Neck, Teach Me Anatomy.com, August, 2023
Recommended Articles
Lymphoedema – NHS (www.nhs.uk)
Lymphatic drainage | The Royal Marsden
Lymph nodes: Purpose, location, and disease warning signs (medicalnewstoday.com)
Lymphatic Dysfunction (Lymphedema): Symptoms and Treatments (healthline.com)

2023-08-29 08:22
On Shame
What Is Shame?
‘Shame is a feeling of embarrassment or humiliation that arises from the perception of having done something dishonourable, improper or immoral. When shame is chronic, it can involve the feeling that you are fundamentally flawed. People who experience shame usually try to hide the thing they feel ashamed of.’[1]

Different Types of Shame
In The Psychology of Shame, Arlin Cuncin speaks about the different types of shame. Chronic Shame is with you all of the time, and makes you feel that you are not good enough. Humiliation is the most intense form of shame and comes about when we are critically embarrassed about something. Shame about the Self is a feeling that you are an inferior person. This is chronic and can have long lasting effects. Defeat. We feel shame when we experience failure or defeat. Internalized Shame is shame that we turn inward and involves feeling unworthy. Lastly, Toxic Shame involves the belief that there is something inherently wrong with you.
‘Shame derives its power from being unspeakable. If we speak shame, it begins to wither. Just the way exposure to light was deadly for the gremlins, language and story bring light to shame and destroy it.’
Brené Brown; Daring Greatly; How the Courage to be Vulnerable Transforms the Way we Live, Love, Parent and Lead.
My Shame

It’s a hard one to admit. For many years now, I have experienced a deep sense of shame about the way that I have been treated by the medical fraternity in the UK. I feel dismissed, humiliated and patronised – humoured, in fact. I also feel a sense of failure. Over this last decade, I have watched friends and peers raise kids, become top-shot barristers and wade through mortgages, whilst my forties have been lost, pleading with doctors.

My forties are a dead decade. There is little to show for them, aside from meeting a lot of Head and Neck Surgeons. I was excited about starting my forties and pursuing a vocation as a writer. My forties opened with me beginning a Master’s Degree in Writing. I was full of optimism about entering the new decade. In just one month, I turn fifty years old. I look back at the decade behind me, and feel enormous sadness about the time that I have lost, trying to get my facial pain diagnosed and treated. I could have built a school, a road, or written ten novels, with the energy that I have used trying to get the medical profession to listen to me.
Shame and Inferiority
‘Frequent experiences of shame may eventually crystallize into trait-like shame proneness. Trait shame, involves a particularly painful, and often incapacitating, negative feeling involving a sense of inferiority.’[2]
My feelings of humiliation are definitely intertwined with a feeling of inferiority. I struggle to understand why this has happened to me. I ask myself if this would have happened to friends, colleagues, or even well-known celebrities? Probably not. I think about mothers who have children. If this was a child of theirs, they would not have stood by, and watched their child live with debilitating pain for ten years. They would have walked over burning hot coals to get their child sorted. I feel that I have failed to self-advocate.


The fact that these consultants won’t give me the time of day, leaves me feeling like I have no worth. Each morning, when I wake up, the first thing that I feel is my left cheek burning. I feel a gnarly, heavy weight, that presses around my left eye. My temple throbs. The fullness and pressure in my ear, muffles my hearing, and the stern pain around the left side of my head dulls me. My body tells me that it is not well. Yet, I cannot get it the medical help that it needs. Therein lies my shame.
‘Shame can be problematic when it becomes internalized and results in an overly harsh evaluation of oneself as a whole person. The inner critic might tell you that you are a bad person or have no value. The truth is, how deeply you feel ashamed has little to do with your worth or what you have done wrong.’
Arlin Cuncic, The Psychology of Shame.
It’s Not About You

My intellect knows that what has happened to me is not personal. It is not to do with what I have done. What has been happening is endemic. The resistance that I have faced from medical professionals about my facial pain is out of my control. It is entrenched within the machinery of these large institutions. I cannot stop medical consultants influencing one another’s opinion of me. Nor can I influence the wheels of corruption that turn behind the four walls. I have been a victim of institutional bullying. One woman, alone, cannot stop fifteen NHS Trusts from behaving in this way.
On Comparison

My feelings of shame intensify when I compare myself to others. It sucks to suffer with a chronic illness in a social media era, where self-promotion and perfection prevails. Bring back the days of The Yellow Pages and curly wire phones. Comparison is the new blight on our culture. Instagram reels are full of picture-perfect lives, which I feel I am limping one hundred miles behind. It is impossible to airbrush being in constant pain.


The core of the humiliation that I feel is that I do not understand why have I been consistently mistreated by so many medical professionals. I blame myself. Is it my fault? Did I do something to elicit this response? No. Has the abuse that I suffered as a child created an open invitation for everyone to give me a beating? Maybe. Or is it an unforgiving system that does whatever it needs to do to protect itself, even at the expense of a patient’s quality of life? Most certainly, yes.
Shame Resilience Theory (SRT)

US Writer and Professor, Brené Brown has been researching shame for two decades. She says that we can move through shame towards empathy by building resilience. We can do this if we learn to develop; 1) Our capacity to recognize shame, 2) Maintain our authenticity and grow from our experiences and 3) Develop stronger, more meaningful connections with people in our lives. Through her research, Brown identified that those able to move through shame, all shared the following elements of shame resilience;
- Recognizing shame and understanding it’s triggers
- Practicing Critical Awareness
- Reaching Out
- Speaking Shame; Keeping quiet and keeping are shame secret are fanning the flame.
Healing From Shame

The Psychology of Shame, explains how shame can make you feel flawed. Shame leads to social withdrawal, to depression and sadness, and can cause other physical problems. Shame can cause lowered self-esteem, anxiety and loneliness, and it can make it harder to trust other people.
Empathy is a hostile environment for shame.
Brene Brown, 2021
Brené Brown speaks about the need to practice self-compassion and self-forgiveness in overcoming shame. Developing self-understanding and being kind to ourselves is a vital component in this healing journey. She speaks about the importance of not being too over critical of ourselves, and she identifies that mindfulness is a useful tool to begin practicing this. My journey to heal from my feelings of shame are going to take a long time. Whilst I am still living with unbearable facial pain, it is difficult to do this, as my facial pain and my feelings of embarrassment are so closely interlinked. I think, if I can find a doctor, who will level with me, and begin treatment for my condition, then the humiliation that I feel about what has happened to me will organically thaw.


My Healing
In order to begin to heal, I must separate the system from the personal. This is not about me, or my failings, or what I have done, or not done. My story is a tragic indictment of our unforgiving system, that fails to see the person beneath the symptoms. The system is broken. It needs rebuilding from the ground up, using care and compassion as cement.

I am a shadow of the woman I was ten years ago. The kicks that the system has given me have scarred me. However, one thing that I do know, is that I have remained dignified throughout this battle. I have never sworn, or been rude to any of the professionals who I have dealt with. I have presented rational arguments to all of the medical professionals who I have seen, and I have been truthful every step of the way. For that, I know I can stand proud.

[1] Cuncin, A; The Psychology of Shame, VeryWellMind.com, June, 2023
[2] Velotti, P, Garofalo C, Bottazzi F & Caretti V; Faces of Shame: Implications for Self-Esteem, Emotion Regulation, Aggression, and Well Being. The Journal of Psychology, June, 2016
Recommended Reading
Shame; A Concealed, Contagious and Dangerous Emotion
Must Watch Video’s

2023-08-22 05:50
On No Advocacy
What Is Advocacy?
The Merriam Webster dictionary definition of advocacy is the act or process of supporting a cause or proposal. A broader definition of advocacy is getting support from another person to help you express your views, and help you stand up for your human rights. Advocacy helps people to speak up and get involved when decisions are being made about their life. Advocates are there to be on your side. Advocacy can involve listening, practical support, like attending meetings, accessing and understanding information, challenging discrimination, communicating choices, protecting human rights, and promoting the person’s wishes and preferences.

One of the most difficult aspects of my ten-year quest to get a diagnosis and treatment for my facial pain, has been the lack of advocacy. Nobody within the system who has listened. There has been no one on my side.

My GP’s
The General Practitioner is our number one advocate. The Ghosting of my General Practitioner explains how my General Practitioners have had a tough time during this medical crisis, due to many of their referrals being rejected by consultants. I have had great sympathy for their position. However, throughout this 10-year episode, none of my GP’s have spoken to the consultants on my behalf. Each time that a consultant dismisses me, the GP remains silent, instead of trying to push through this barricade that I face.

A GP can only refer a patient to secondary care. They have limited power. I know that. However, Good Medical Practice states that a doctor ‘must work Collaboratively with colleagues,’ (35.) There has not been any dialogue between my GP’s and these consultants. Each GP that I have had during this health episode has left me to carry the burden alone. All I have wanted is for them to carry some of the weight.

I have shown my GP my scans. He said that he can see that there is something ‘seriously abnormal,’ but, he writes, scan abnormal-to be expected-no action needed, in my notes. Even when he sees that there something wrong, he keeps quiet. The same is true for other statutory services. No matter who I turn to within the system, when they see how many NHS Trusts have been involved, they say; ‘Sorry there is nothing I can do.’ No one wants to upset muddy waters, but it is too heavy a burden for me to carry alone.

The Process
After my GP refers me, I wait, on average 4 months for a hospital appointment. I sit in the clinic waiting room. Homes Under the Hammer is showing on an overhead television. I read over my notes to make sure that my questions are clear in my head. In my imagination, Danny Dyer sits on one shoulder and Piers Morgan on another, two people, who would not take any c**p. I affirm to myself, that this time, I will stand up for myself.
The Consultation
The tone of voice with which the Consultant calls my name, says it all, as does the look that he gives me. Even before I have sat down on the horrid orange chair, I feel that lump in my throat. He sits back in his chair, legs crossed, with his chin, resting in his hand. ‘Fire away,’ he says, ‘tell me about the pain.’
I start to speak, while he taps his pen on his desk. My voice is small. I make the mistake of mentioning the previous hospital, where I was seen.
‘Who did you see at that hospital? he asks.
I don’t mention the name of the consultant.
‘Which hospital was it again?’
I repeat the name of the hospital. He takes in a big gulp of air and raises his eyebrows. ‘You have been around, haven’t you?’
‘Yes, I have,’ I reply, finding more power in my voice.
I stupidly mention that I have seen the most senior Head and Neck surgeon in the UK.
‘Well if you have seen Professor Pompidou, how do you expect me to help you?’ he asks.
Professor Pompidou didn’t want to help me. He told me to ‘stop chasing the dragon,’ that ‘he was only interested in life-or-death cases, not a bit of obstruction in the parotid gland.’ I don’t tell the consultant this. I keep quiet and look at the floor.

The Examination
‘Can I examine you,’ he asks? He puts on his latex gloves, and feels the back of my neck. ‘Everything feels normal,’ he says.’
‘That’s not where I have the pain,’ I reply. ‘It’s here.’ I point to the left side of my face. ‘It’s in my cheek and around my eye.’
He crumples up his eyes, returns to his desk, and jots down some notes in his file. ‘Have we done any bloods?’ he asks.
‘My GP did some two weeks ago. My infection markers were raised, again.’
He scans his computer screen. ‘Yeah, but not by much,’ he says.
‘They’ve been raised like that for ten years,’ I say.
”That doesn’t mean a lot.’ He holds his biro between his lips. ‘We need to do a wait and see approach.’
‘And what does that involve?’ I ask.
‘We’ll monitor it, and wait for you to get really ill. Then we’ll do something.’
My cheeks become flushed. I stand. I need to get some air.
He extends his hand to shake mine. ‘It’s been lovely to meet you,’ he says with a plastic smile.
I slide my hand into my pocket. ‘Goodbye,’ I say and rush out of the door. I know that another dismissive letter is on its way back to my GP.
Where did Danny Dyer and Piers Morgan go?

Post-Consultation
I come out in deep shock. I pace up and down the hospital grounds, ponce a cigarette off a stranger, which I justify smoking, because I need to tame the shock. That makes me feel sick. I sink into myself, as scenes replay through my mind of his condescending tone. We’ll wait for you to get really ill. The level of alarm that I experience is like someone has just mugged me.

I become quiet. I cannot speak or cry. My mind is jumbled with self-persecuting thoughts. Why did I let it happen to me again? It takes weeks to process the reverberations. My GP shrugs and says; ‘I am sorry that it has happened again, Felicia.’ I speak to the Mental Health team. A lady tells me that I ‘need to reframe the way that I view the situation.’
Reframe it?

No Responsibility
Telling me to reframe the situation is putting the responsibility back onto me. This is not my responsibility to carry. She is asking me to shoulder someone’s else’s failing by ‘changing my viewpoint.’ Dangerous. I call the Crisis team. They tell me that their ‘hands are tied.’ I feel myself sink. My head slips beneath the water.

There have been 60 plus scenarios similar to the one that I have just painted. On Gaslighting speaks about how victims of gaslighting become increasingly emotional as a result. This can make them more likely to be seen as having unreliable judgement, which discredits them further. Instead of understanding that I am in distress because I am in acute physical pain, and nobody is listening, these consultants see the distress as the problem. They fail to understand the impact that both my facial pain and their behaviour are having on me and my mental health.
Patient Advice Liaison Service

Patient Advice Liaison Service, (PALS) is a service to help patients resolve concerns within the NHS. It is available within all NHS Hospitals, to provide support with problems that one has not been able to resolve with a ward or with staff in a clinic. They also provide assistance with the NHS complaints procedure. I have reached out to PALS on a number of occasions, with issues that I have had with various clinical teams. I have never received any satisfactory help or resolution from them. They just signposted me to the NHS complaints procedure, which I did not find fruitful.
Independent Advocacy Services
There are many independent advocacy services within the UK. My experience of using these advocacy services has not been great. One advocate, cancelled attending the medical appointment with me ‘because it was too early in the morning.’ The other advocate was more terrified of the authorities than I was. However, many people speak highly of advocacy services, that I have not used. PohWer is an organisation, that provides help with NHS Complaints advocacy and independent mental health advocacy. Voice Ability is an independent charity, that supports people to be heard in decisions about their health, care and wellbeing, and Advocacy People also provide mental health advocacy and independent care act advocacy. Lastly, Mind provide information about advocacy support for people with mental health difficulties.
Conclusion

We need a patient advocacy service within the NHS, which is separate from PALS. There needs to be professional advocacy support for adults, who struggle to get heard within the medical system. Patients need trained advocates, who have the time to get to know the patient and their case. Patients should not feel this frightened and alone. We need advocates to help us navigate the system and help our voices be heard.
If I had been assigned an advocate, who was on my side, and had fought for me to get heard, then I am certain that I would have been diagnosed and treated for my facial pain by now. The NHS must integrate a patient advocacy service, within every NHS Trust, to ensure that other patients don’t waste ten years, like I have, trying to get heard by a system that is refusing to listen.

Resources
Someone to speak up for you (advocate) – Social care and support guide – NHS (www.nhs.uk)
What is Advocacy? – Advocacy Focus
Mind- Advocacy in Mental Health
Useful Videos

2023-08-15 06:14
Follow The Leader
This blog post contains wording about suicide that some people may find triggering. If your need is urgent, please call 999. If you need support, please call 111, or The Samaritans freephone helpline on 116 123. Stay safe.
The Game
Follow the Leader. This is how it goes. A lady lies face down in a ditch. She is covered in blood. A swarm of fly’s circle around her. She cries for help. A businesswoman, who is late for a meeting, strides past. She sees the lady in the ditch, but she walks on by. No one will notice. A banker follows behind. He sees the woman in the ditch. He has a wife to get home to. Mr banker spots the woman who walked on by in front. She did it. I’m OK to do it too. He picks up a pace and marches on.
Tens, hundreds, and then thousands follow suit and walk on by. They ignore the woman in the ditch. They are OK to leave her where she is. There is safety in numbers.

Ten years pass. One full decade. This poor woman is still in the ditch. People continue to pass her by. It is permissible behaviour. So many people have ignored her, that it is acceptable for everyone else to do the same. The stranger in front grants permission to the person behind to walk by. Like sheep, they follow.

The Woman’s Reality
The system has failed her. Fifteen NHS Trusts, nine General Practitioners, four Mental Health Teams, three Crisis teams, and two local authorities have walked on by, and left her in the ditch. The specifics are shocking. Fifty plus Medical Consultants have pushed her away and closed her case. There is nothing wrong with you, stupid woman. Stop banging on about your face and live with the pain. Nine GP Practices have buckled. We can’t do anything- Sorry. If all of these Consultants are ignoring you, then it is safe for us to turn a blind eye, too. They stay quiet and do nothing.

Mental Health Services
The lady reaches out to the mental health services for support. She makes a loud cry for their help.

They follow suit. We are not going to stick our head above the parapet and get shot. If all of these NHS Trusts have washed their hands of you- we can get away with it too. We don’t want to be seen to be supportive. The mental health team tells her that she needs ‘to reframe the way she sees being in the ditch.’ They throw a blanket over her and walk on.
Social Services
The lady has been open to Social Services since 2008. Several passers-by have raised causes of concern to Public Protection about this lady in need. No one from social services bothered to see if she was OK. A new Local Authority have taken over her case. They have assessed her as having care needs under The Care Act 2014. They know how many NHS Trusts have knocked her back. Two social workers go down to the ditch one day. ‘You’re doing just fine in the ditch, alone,’ they say. You don’t need our help anymore. You can do it on your own.’ They withdraw their support and close her case.
This mass abandonment hurts her so deeply. She cannot endure the pain anymore. The lady feels that the only way out is to be dead. She fights the urges to end her life. She does not want to commit an act of murder. One day, she manages to limp to the local Accident and Emergency department to speak to the Crisis teams. She tells them that being in the ditch, is making her want to end her life. The lady tells explains that she cannot stay in the ditch any longer.
The Crisis team look in her notes and see the long line of NHS Trusts and services who have ignored her. They don’t want to go against the grain. They tell her that she should go back to the ditch and ‘distract herself.’
It’s an endemic game of Chinese Whispers.

Thomas Kuhn on Paradigm Shift
Thomas Kuhn was an American historian and philosopher of science. His book, The Structure of Scientific Revolutions was published in 1962. It is about the history of science, and it was very influential in academic circles. It introduced the term paradigm shift, which has since become an English-language idiom. I discovered this book in my final year at university, during a course that I took in Comparative Epistemologies. This book is one of the few things that I still remember from my degree. It caused me to think in a different way about a lot of things.

‘Thomas Kuhn argued that science does not evolve gradually towards truth.’[1] ‘The Structure of Scientific Revolutions argues that the development of science is driven by adherence to what Kuhn called paradigms.’[2] A paradigm is a basic framework of assumptions and principals, from which members of the community agree upon. It is a set of norms that tell scientists how to act and behave.
Scientists accept the dominant paradigm until anomalies are thrown up, when scientists will then begin to question the basis of the paradigm. New theories emerge, which challenge the dominant paradigm and eventually, one of these theories is accepted as the new paradigm.
Thomas Kuhn’s Series of Phases
Thomas Kuhn states that discoveries of scientific theories are based upon a series of phases.
- Phase 1- Pre-Science; Scientists explore different theories. They have not yet arrived at a model to follow.
- Phase 2- Normal Science; Scientists work together on a common question. They carry out their work on the basis of a paradigm. In order to arrive at the paradigm, a number of assumptions are explored, and when there is enough agreement between them, a paradigm is formed.
- Phase 3-Crisis Phase; Anomalies and irregularities arrive and need to be solved. Abnormalities keep piling on, and this is when a paradigm shift begins. The crisis phase is when scientists question the model and its feasibility. It then enters a new stage where the entire paradigm on which everything is based needs to be shifted to a new one.
- Phase 4- Revolutionary Phase; A completely new paradigm is formulated, which is not the result of the old paradigm. It is formulated with the help of new observations, and it draws on new perspectives.
Conclusion
My case is not scientific theory- I know that -but I do draw a parallel between Kuhn’s theory of paradigm shifts and my story. The existing paradigm is based on an agreement between many statutory bodies, that ignoring me and treating me badly is acceptable behaviour.
Anomalies and irregularities have been showing up with this paradigm for a long time. It has reached crisis point. I now have six entries of suicidal ideation on my medical records. I also have an active request for an accompanied suicide, pending with Dignitas in Switzerland, which I have made on the grounds of uncontrollable and unbearable pain. It is time for people to question the feasibility of the existing paradigm. It’s foundation is flawed, and is based on hurtful behaviour, which is causing me considerable harm. We need a paradigm shift.
In order for a paradigm shift to occur, it will take a courageous person, who will stop and see this lady. They will help her out of the ditch and accompany her to a hospital, where she can receive medical treatment for her facial pain, and support to help her heal from the trauma. If this person shows her kindness, others will follow. The old paradigm of neglect will be replaced with a new model of care and compassion.
This lady will not survive being in the ditch much longer. It is time for somebody to stop and give this lady a hand, so that love and healing can replace this toxic culture of neglect and duplicity.

Back To The Lady
The lady waits in the ditch. She clings to the burning embers of her late mother’s legacy, that by the laws of averages, nothing can stay at an extreme for ever. Her father used to read her fairy tales when she was a child. She thinks about those stories; how a dawn of love and humanity emerges at the end of a dark tale. Her story has been dark. Over the last decade, she has seen the worst of people, but she has clung to universal truths, maybe cliches, that good overcomes bad in the end.
The lady lies awake at night and asks herself the same questions. When will things balance out? When will compassion and humanity appear, and how much longer does she have to wait for someone to help her out of the ditch?

Recommended Articles
Thomas Kuhn and the Structure of Scientific Revolutions
The Structure Of Scientific Revolutions
Thomas Kuhn: The Man who Changed the Way the World Looked at Science
Abuse of Power; The psychology behind Abusive Relationships.
Foot Notes
[1] Mcleod Saul PhD; Thomas Kuhn; Paradigm Shift. June, 2023- Simply Psychology.
[2] Sack, Harold, Thomas Kuhn and the Structure of Scientific Revolutions, July 2021, SciHi Blog; Daily Blog on Science, Tech and Art in History.

2023-08-09 09:38
Good Medical Practice #3
Summary
My facial Pain is a quest to find answers about my condition. It is also a quest to find answers about how such a radical deviation from Good Medical Practice, by so many consultants, across so many NHS Trusts has gone unregulated for a whole decade. Good Medical Practice #3 reflects on whether there is enough regulation of doctors, who practice within the UK.

Guidance not Rules
McManus, Gordon and Winder explain in their article; Duties of a Doctor: UK doctors and Good Medical Practice that GMC guidance is ‘in effect a definition of best quality medical care, against which the performance of a doctor can be judged. Its role is advising on the basic principles of good practice. It is only guidance. It is not a set of rules, nor is it exhaustive.’[1]
McManus, Gordon and Winder recount an experiment, that was conducted, where questionnaires were sent to 794 doctors. The questionnaire asked how much the doctors knew about Good Medical Practice. ‘Eighty-nine per cent of doctors acknowledged that they had received a copy of Good Medical Practice, however only 17% of doctors had read it carefully.’[2]
This is an extremely low percentage of doctors, who seem familiar with Good Medical Practice.
Reflections

I have walked out of so many consultations in tears. This is because a consultant has been either dishonest, rude or disrespectful. I have asked myself whether they would have behaved that way if a member of the British Medical Association or General Medical Council had been watching the consultation. If there had been surveillance from a regulatory body, I do not believe that they would have spoken to me like this. If The British Medical Association or General Medical Council made unannounced visits to consultations, like the Care Quality Commission do with unannounced inspections, things could potentially progress. More supervision could foster greater adherence to GMC guidelines by medical professionals.

Does the General Medical Council assume, that because consultants and surgeons reside within an intelligence sphere that many of us don’t touch the sides of; that they are immune from having to follow GMC guidance? I do not understand why there is not more regulation of doctors, or more effort made, to at least ensure that all doctors are familiar with Good Medical Practice. Greater regulation is needed. There needs to be stricter rules to ensure that all medical practitioners are abiding by GMC guidance. Good Medical Practice is in place to protect public safety. The GMC has a duty, therefore, to make more stringent enforcement of these guidelines.
On Humans

As humans, we are all capable of behaving badly and not following guidelines. Look at the Pandemic Government. Most of its shining stars have gone, minus Rishi Sunak. They have gone because they broke their own rules. They did not tell the truth. The public lost trust in them. The lasting image for me, of the Pandemic Cabinet was, Queen Elizabeth, sitting alone, in a cubicle , at her husband, Prince Philip’s funeral, whilst Matt Hancock, the then Health secretary, was snogging his aide behind closed doors, at The Houses of Parliament. It reeked.

Doctors are not exempt from the human ability to behave badly and deviate from guidance. There must, therefore, be greater regulation to ensure that all medical professionals, even those who are highest up the ladder, adhere to Good Medical Practice, in order to keep the public safe.
Conclusion
McManus et al, state how there has been increasing publicity about errors and malpractice of hospital physicians and general practitioners. They explain that ‘the medical profession in the UK is currently self-regulated. There have been fears that unless the General Medical Council (GMC) responds to growing public fears, the self-regulation of doctors may not be sustainable for too much longer.’
I would argue, from my experience over the last decade, that it is time to move on from self-regulation of doctors. We need doctors, who we can trust. There needs to be stricter regulation of conduct within clinical settings, to ensure stories like mine do not repeat themselves. It is time to move towards stricter surveillance of medical professionals, to ensure that the public are kept safe.

Recommended Articles
Good Medical Practice guidelines
Foot Notes
[1] McManus, IC, Gordon D, Winder BC; Duties of a doctor: UK doctors and Good Medical Practice, P14, Quality in Healthcare, 2000
[2] McManus, IC, Gordon D, Winder BC; Duties of a doctor: UK doctors and Good Medical Practice, P18, Quality in Healthcare, 2000

2023-08-08 08:47
On Good Medical Practice #2
Summary
During my quest to find treatment for my facial pain, I have been stunned by many medical consultants, have, in my opinion, deviated from Good Medical Practice. I have seen over fifty consultants across 15 different NHS Trusts. It would not be possible to cite all of the examples. I will cite a cross-section of examples of deviation of Good Medical Practice, which span across its four domains.

Deviation Example 1
I saw a Head and Neck surgeon at an NHS Trust in Scotland, regarding my left sided facial and peri ocular pain. He promised to do a set of new scans, discuss my case at a Multi-Disciplinary Team meeting, and refer me to ophthalmology and Infectious Diseases. He told me that he would see after the scans, to ‘find a way forward.’ After I had my MRI and CT Neck scans, I received a letter from him saying, that he wanted to explore the ‘pain management’ route. Weeks and months went by. The consultant made no contact with me. I wrote to him three times, and asked for a follow up appointment. I did not receive a reply. There was a long silence.

He referred to me to a Pain Management team, who wrote back to the surgeon to say that they could not accept me onto their service, because ‘I was not suitable for their service.’ The surgeon referred me to an Infectious Diseases consultant, who saw me once. My infection markers: neutrophils and white blood count, were both raised in the blood tests that the Infectious Diseases Consultant did. However, he discharged me, in spite of these abnormal raises. He left me with no follow up care or treatment.
Dead End

There was no contact from the Head and Neck surgeon for eighteen weeks. I heard nothing from him, so I wrote to the NHS Trust, and I explained to them that I had not been given a follow up consultation with the surgeon. I received a letter from the NHS Trust, saying that I needed to be seen by Pain Management. The NHS Trust wrote this letter to me in knowledge that the Pain Management service had rejected the surgeon’s referral. They sign posted me back to a service, who they knew had declined to see me. I was led down a dead end.
Three clinical teams; Infectious Diseases, Pain Management and Head and Neck surgery, all declined to help me. They gave me no adequate explanation as to why. I had three doors shut on me, when clinical data: scans and blood tests, were available, and which showed that there was something clinically wrong. They overlooked this clinical evidence and left me with no care. I found this difficult to understand.
Communication, Partnership and Teamwork

Good Medical Practice states that a doctor ‘must’
(3) 31 Listen to patients, and respond honestly to their questions.
(3) 32 Give patients the information they want or need to know in a way they can understand.
I wrote to the Head and Neck surgeon, four times asking him questions about the scans. I received no reply. The same applied with the Infectious Diseases consultant; I wrote to him, and asked what the abnormal raises with my neutrophil and white blood count indicated. He did not respond to me either. Neither of them ‘answered my questions honestly’ or ‘gave me information that I wanted and needed to know about my condition.’ Both instances seem like a clear departure from Good Medical Practice.
Good Medical Practice states that a doctor ‘must’
(3) 35 Work collaboratively with colleagues, respecting their skills and contributions
(3) 44.a Check, that a named clinician or team has taken over responsibility when your role in providing a patient’s care has ended.
There was no collaboration between these clinical teams. The Head and Neck surgeon knew that Pain Management had refused to see me, yet he signposted me back to them. The surgeon was also aware that Infectious Diseases had discharged me. He closed my case, without ensuring that there was anyone to take over my care. He ghosted me for twenty-four weeks. It was painful. His behaviour made me feel insignificant and invisible.

Deviation Example 2
I recently published two blog posts, in which I spoke about consultants, who made offensive comments to me and spun the truth, when I asked them about radiology images. One consultant told me to ‘stop shopping around.’ Another told me to stop ‘chasing the dragon.’ I asked an Oral Maxillofacial consultant to explain visible facial asymmetry in a CT scan. He answered by telling me that the quality of my iPad was s**t.
A third Oral Maxillofacial surgeon told me that the asymmetry in the scans was because my face ‘was lopsided in the scanner,’ when he had not seen me go into the scanner. Another consultant told me that it was just ‘coincidence,’ that what I was seeing in the radiology image, was where I had pain. That same consultant then went on to photoshop radiology images, in front of me, so that the abnormality disappeared. It was beyond shocking.

Good Medical Practice states that a doctor ‘must’
Establish and Maintain partnerships with patients
(3) 46 Be polite and considerate
(3) 48 Treat patients fairly and with respect
(4) 65 Make sure that your conduct justifies your patients’ trust in you and the public’s trust in the profession
(4) 68 Be Honest and Trustworthy in all your communications with patients and colleagues
Their behaviour was not ‘polite’ or ‘considerate.’ I was not treated with respect or fairness. Their communications were not trustworthy, and their conduct failed to justify my trust in them as doctors, or in the profession at large.
Deviation example 3
I had an MRI Neck scan done at an NHS Trust in Yorkshire, in July, 2021. The radiology report states that abnormality has been detected. The abnormality found, relates to the Buccal Fat Pad and retromolar region, on the left side of my face. I have asked four different clinicians at the hospital, what the abnormality is. I have received no explanation. There has been no follow up in regards to explaining what this abnormality is, or treating the abnormality. I am in severe and worsening pain, and yet there is ‘evidence available’ on file, at a hospital, which shows that something is clinically wrong. Nobody has acted on it.

Knowledge, Skills and Performance
Good Medical Practice states that a doctor ‘must’
(1) 15 Provide a good standard of practice and care. If you assess the patient, you ‘must
b Promptly provide suitable advice, investigations or treatment
16 In Providing clinical care you must;
(1) b Provide effective treatments based on the best available evidence.
There is ‘evidence available,’ that there is an abnormal process going on in the soft tissue of my face. The NHS Trust have not ‘promptly arranged treatment,’ or ‘provided effective treatment based on the evidence available.’ I have asked what this abnormality is. They have not ‘responded honestly to my questions,’ or ‘given me information that I want and need to know.’ ( Good Medical Practice; 31 and 32)
I had a similar experience, when I was a patient at a salivary gland unit at an NHS Trust in London. They found, via ultrasound and sialography, that my salivary gland was not functioning properly. The clinic detected obstruction in my parotid gland. I was having saline wash outs, which they promised to do long term. However, they suddenly discharged me from the clinic, for no reason, and in spite of them having clinical evidence available that there was something wrong.
Deviation example 4
A recent blog post, The Ghosting of my General Practitioner, explains how nine different GP practices have sent out referrals, which have been refused or irresponsibly batted back to the GP. My current GP referred me to an Oral Maxillofacial department. They sent the referral back because the problem was too ‘complex.’ My GP was advised to send the referral to a named clinician a Teaching Hospital. He did this. We did not hear anything for months. I telephoned the hospital, and I was told that my case had been closed; that I had been discharged, without being seen. They did not inform my GP of the rejected referral. Again, this conduct was beyond shocking

Good Medical Practice states that a doctor ‘must’
(3) 35 Work collaboratively with colleagues, respecting their skills and contributions.
36 Treat colleagues fairly and with respect
44 a Share all relevant information with colleagues involved in your patients’ care within and outside the team.
For the Oral Maxillofacial department to not even inform my GP that they had rejected his referral is neither, ‘working collaboratively,’ ‘treating him fairly or with respect,’ or ‘sharing relevant information’ with him. This is a major divergence from Good Medical Practice.
Conclusion
I have attended 60 plus consultations over the last ten years regarding my left sided facial pain. I have over fifty letters, saved on my desktop, which I have written to consultants, asking questions about my condition. None of them have responded to me. The questions that I have been asking is a) why the oral antibiotics work up to a point, but when I come off them, my symptoms return, b) what the abnormal raises in my bloods indicate, and c) what the aetiology is behind my facial pain.
What I struggle with most deeply, is that there is clinical evidence available, which holds valuable information about the possible pathology behind my medical problem. However, numerous consultants ignore the data. The data, which I wish they had paid attention to over the years, are my blood test reports, which have shown raised infection markers since 2013. There have also been scan reports and histology reports, which have show abnormality, which have been overlooked. This seems to be a departure from Good Medical Practice, which states that doctors ‘must’ ‘provide treatment based on the available evidence.’

The Rejection Hurts
What has hurt the most, is the ruthless way that clinicians have shut my case down, before they have even met me. I have been perplexed why so many referrals have bene rejected and why I have been prematurely discharged from so many clinics, when there is ‘evidence available’ that there is a clinical problem. Throughout my entire ten-year battle to get treatment, most of the consultants who I have seen have discharged me after one appointment. They have not taken ‘all possible steps to alleviate pain and distress whether or not a cure may be possible.’ (Good Medical Practice, (1) (16 c) In fact, quite the opposite. Their dishonest and offensive behaviour has created more distress and further confusion.

Recommended Articles
The Ghosting of my General Practitioner
Good Medical Practice- GMC Guidance

2023-08-07 07:26
On Good Medical Practice #1
Summary
The General Medical Council, |(GMC) is an independent regulatory body for the medical profession in the UK. It is responsible for overseeing licensing, training, registration of doctors, and setting standards of Good Medical Practice. It also investigates concerns to maintain patient safety. The function of The General Medical Council, is to protect, promote and maintain the health and safety of the public.
Good Medical Practice is a document, which is published by the UK’s GMC. The document describes what is expected of all doctors, who are registered with The General Medical Council. It sets out the standards of competence, care and conduct set by the GMC, and it is the responsibility of doctors, who are registered with the GMC, ‘to follow the guidance it contains.’

‘Patients need good doctors. Good doctors make the care of their patients their first concern: they are competent, keep their knowledge and skills up to date, establish and maintain good relationships with patients and colleagues, are honest and trustworthy, and act with integrity and within the law.
Good doctors work in partnership with patients and respect their rights to privacy and dignity. They treat each patient as an individual. They do their best to make sure all patients receive good care and treatment that will support them to live as well as possible, whatever their illness.’[1]
The Duties of a Doctor
In Good Medical Practice, the GMC sets out the professional standards that are expected of doctors: values, knowledge, skills and behaviour.
‘Patients must be able to trust doctors with their lives and wellbeing. To justify that trust, we as a profession must show respect for human life and make sure that your practice meets the standards of you in four domains.’
As a doctor you ‘must’:
1. Knowledge, skills and performance
Make the care of your patient your first concern
Provide a good standard of practice and care
Keep your professional knowledge up to date
Recognise and work within the limits of your competence

2. Safety and Quality
Take prompt action if you think that patient safety is being compromised.
Protect and promote the health of patients and the public.

3.Communication, partnership and teamwork
Treat every patient politely and considerately
Treat patients as individuals and respect their dignity
Respect patients’ right to confidentiality
Work in partnership with patients
Listen to, and respond to their concerns
Give patients the information they want or need in a way they can understand
Respect patients’ right to reach decisions with you about their treatment and care
Work with colleagues in the ways that best serve patients’ interests

4. Maintaining Trust
Be honest and open and act with integrity
Never discriminate unfairly against patients or colleagues
Never abuse your patients’ trust in you or in the public’s trust in the profession.
You are personally accountable for your professional practice and must always be prepared to justify your decisions and actions.
The Duties of a doctor registered with the GMC.[2] This extract appears on the inside front cover of Good Medical Practice.

Useful Videos
Below are two you tube videos, which explore in depth, what is expected of a doctor, and what General Medical Council guidance involves. The document: Good Medical Practice is available to view, in full in the download section of my website.
Useful Links
Good Medical Practice guidelines
Good Medical Practice: Public Consultation
Foot Notes
[1] General Medical Council; Professionalism in action, P4 Good Medical Practice, Published, London, 2013
[2] General Medical Council, The Duties of a doctor registered with the GMC, Good Medical Practice, London, 2013

2023-07-25 09:02
Reflections on Gaslighting
Summary
Reflections on Gaslighting draws on The British Medical Association’s; ‘Doctor-Patient Relationship Toolkit,’ which I will be using to reflect on the incidents that I wrote about in my two recent blog posts about being gaslighted by medical consultants. In this Toolkit, The British Medical Association (BMA) clearly sets out the legal requirements, rules and principles, relating to the doctor-patient relationship, which health professionals are encouraged to use, when faced ethical decision making.
‘Good doctor-patient relationships are characterised by mutual respect, open and honest communication, and respect for the dignity and choices of patients.’
Key Principles

The British Medical Association, (BMA) states that ‘the onus is principally on the health professional to make the contact with patients work well. The basic principles underpinning the doctor-patient relationship are;
- Treating one another with respect and honesty, although doctors have particular duties to patients rooted in their professional status.
- Doctors must make the care of their patients their first concern.
- Good communication requires openness, honesty and an ability to listen.
In key patient-facing principles, the BMA says that in the guidance set out by The General Medical Council, (GMC) in Good Medical Practice, doctors ‘must,’
- Make the care of the patient their first concern.
- Treat every patient politely and considerately.
- Listen to patient’s and respect their views.
- Give patients information in a way that they can understand.
- Be honest and trustworthy.
The Duty of Care
The BMA explains in it’s Toolkit that doctors have a legal and ethical duty of care. ‘A duty of care is an ethical, legal and professional obligation to promote the health and well-being of patient’s whilst they are in their care. This means acting in the best interests of patients, and not acting, or failing to act, in a way that causes harm.’ It identifies that The duty of care begins when a doctor or other health professional engages with a patient and continues until one party ends the relationship.
‘Legally, health professionals have a duty of care when they assume responsibility for the patient, such as when a patient is added to a general practitioner list. In secondary care, it may be acceptance onto a caseload.’
Communication and Honesty

In the chapter, Communication and Honesty, the BMA clearly states that good communication and honesty between health professionals and patients are fundamental to Good Medical Practice. It says; ‘Good communication is about establishing positive inter-personal relationships, as well as exchanging information. A failure to appropriately communicate can not only result in conflict, and a breakdown of trust between the patient and the health professional, it is a significant factor leading to patient harm.’ The four most common communication failures by doctors that led to patient harm were;
- A failure to provide patients with appropriate information.
- A failure to keep colleagues informed/sharing of an appropriate level of information.
- A failure to listen to the patient.
- A failure to work in partnership with the patient.
The British Medical Association says that factors for good communication are hearing and understanding patient views, which is a vital part of the doctor-patient relationship. It’s guidance states that health professionals can demonstrate effective and respectful communication with patients by;
- Exploring the patient’s understanding, thoughts and worries about the problem and taking the patient’s input seriously.
- Being approachable and friendly.
- Showing genuine care, and being respectful.
- Being specific and checking patient understanding.

My Experiences
In my two recent posts, Medical Gaslighting #1 and #2, I outline incidents, in which consultants spun the truth when I asked them questions about radiology images. I was asking rational questions, in an attempt to better understand my condition. On leaving these consultations, I felt terrified and was left questioning my own judgement. During these consultations, I did not feel that the consultants treated me with respect or honesty. They certainly did not make the care of me, the patient, their primary concern. They seemed to make colluding with their colleagues’ opinion of me their primary concern.

In summary, these incidents included; 1) A consultant telling me that an image of my face was my spine, 2) A consultant telling me that what I saw on his computer screen was a figment of my imagination, and 3) A consultant in England telling me that a CT image from a scan, done in Scotland, which showed visible facial asymmetry was because my ‘face was lopsided in the scan machine.
The final incident involved a consultant refusing to explain to me what the abnormality, that had been detected on an MRI scan and written in a radiology report, meant. The consultant went on to tell me that what I could see in a scan image was ‘coincidence.’ Most alarmingly, he told me that the quality of my iPad was s**t, when I asked him to explain the visible facial asymmetry in CT radiology images, which I have been trying to get answers to since July, 2021.
Reflections

None of these behaviours, summarised above, adhere to the BMA guidance. There was no open and honest communication. Every question that I asked, I was shut down. The consultant, who told me that my facial asymmetry was because my head was ‘lopsided in the scanner,’ did not see me go into the machine. He knew as well as I did, that that was not true. This example is one of neither ‘open’ nor ‘honest’ communication. Nor is the example of the Oral Maxillofacial surgeon in Scotland, who told me that my face was my spine. This was inaccurate information. It was not trustworthy behaviour.
The BMA draws on the GMC’s Good Medical Practice, which says that a doctor ‘must’ treat every patient politely and considerately and give patients information in a way that they can understand.’ The incident in which a consultant told me that the quality of my iPad was s**t was rude and offensive. I also found the consultant telling me to ‘stop shopping around,’ deeply insulting. Neither examples are of polite or considerate behaviour.
The consultant telling me that the clear abnormality in a scan image was due to ‘coincidence,’ was not being honest. Going on to then photoshop the images, so that the data on the scans changed is far from trustworthy behaviour. It is decidedly dishonest. I did not receive any answers from him about the abnormality, that was reported from my MRI scan. I still have no explanation about this detected abnormality. The consultant was withholding information from me, not ‘sharing an appropriate level of information,’ as he was supposed to do.
Impact of Gaslighting

These incidents did not involve the consultants being approachable, friendly or specific. I felt terrified when I was in the room with them. On leaving all of these meetings, I was in a state of despair and confusion. I also felt undermined. The consultants neither ‘listened’ to me, nor ‘respected’ my views. They all raised their voices. Their failure to communicate with me honestly and respectfully, or give me information that I asked for, not only led to a breakdown of trust, but it caused me considerable harm. My distress levels were acute, and I have since become withdrawn and low in mood.
I have been left traumatised from these incidents. Gaslighting incident number 4 has taken me many months to recover from. It has involved me being unable to sleep at night, getting repeated flashbacks, and it has left me feeling isolated. I have felt decidedly powerless and unable to tell anyone what happened. Fear is the word that best describes how I have felt during and after these gaslighting incidents. Nothing of what I experienced adheres to the BMA guidance, as cited in their ‘Doctor-Patient Relationship Toolkit’ about how to foster positive relationships with patients.
Conclusion

In an article, called Turning Down The Flame on Medical Gaslighting, Shravani Durbhakula and Augustus Fortin, explain that in order to turn down the flame on medical gaslighting, medical professionals need to do a better job of exploring the ‘biopsychosocial model with patients.’ The article argues for a need to focus on relationship-centred communication.
Patients who feel heard, understood, and cared-for will not feel gaslighted; and with proper dialogue, it is more likely that physicians will order the right tests and therapies when they are indicated. Over 40 years of research have shown that using relationship-centred communication skills achieves this, and more5,6. These skills are linked with improved health outcomes and better patient experience. Importantly, these skills can be incorporated into practice with modest effort. Key evidence-based skills include collaborative agenda-setting for the encounter, allowing patients to describe their symptoms without early interruption, eliciting the emotional context of that story, and responding with verbal empathy.[1]
Jennifer Huizen, writes in Medical News today that ‘over time, a person who is a victim of gaslighting may start to believe that they cannot trust themselves, or that they have a mental health disorder.’ This may lead to:
Jennifer Huizen states that all of these can have a long-term impact on someone’s mental health and self-esteem. They may also make it more difficult for the individual to leave an abusive situation.

Foot Notes
[1] Durbhakula, S and Fortin, AH; Turning Down The Flame on Medical Gaslighting, The Journal of General Internal Medicine, July, 2023.
Recommended Articles
How To Spot Medical Gaslighting
Medical Gaslighting; The Women Not Listened To.
Turning Down the Flame on Medical Gaslighting
The Doctor-Patient Relationship Toolkit

2023-07-19 03:07
Medical Gaslighting #2
The Scenario
You are a woman and you go to the emergency room with a severe cough and the ER doctor listens intently at first and acts nice. However, the physician sees on your record that you have a mental health condition or that you have complained about this same problem before. Suddenly, the physician changes with you, and tells you nonsense such as you need to drink more water and the cough will go away. You leave the hospital feeling ashamed, with your self-esteem badly bruised. You feel a fool for ever approaching a medical person for help in the first place and you question yourself and your perceptions, asking yourself, ‘Is it all in my head?’ You have been medically gaslighted and the doctor has committed iatrogenesis.[1]

Gaslighting Incident 3
I was still on a quest to find answers about the CT Neck images from Scotland. I returned to England. My new GP referred me to an Oral Maxillofacial surgeon at an NHS Trust in Northern England. He quizzed me like I was in a police enquiry for an underground bank robbery. I presented the CT radiology images to the surgeon and asked him to explain them.
‘They’re all normal,’ he said. ‘Normal.’
‘These ones,’ I probed. ‘Please can you explain what all of this asymmetry and white is then?’

Figure A

Figure B

Figure C
‘Your face is lopsided in the scanner,’ he said. ‘That’s all that is. You were tilted when you went in.’ He said it with a swagger and he wore a joker like smile.

These scans were done in Scotland, not England, so how could he know if my face was lopsided or not? My head was not tilted or lopsided. My head was placed onto a headrest, with a hole in the middle. There were cardboard wedges, that looked like doorstops, lodged in front of my ears, to keep my head straight.

I tried to fight my corner, but I was petrified. I had no chance. The two nurses in the room looked terrified, too. They sat with their backs to the wall, like they were under arrest. As the consultation ended, it was his final remark that decimated me.
‘You need to stop shopping around,’ he said. ‘You need to accept your pain, and just live with it, Felicia.’
Shopping around? I have been going to see this many clinicians because NHS Trusts keep closing my case. This is my health that I am trying to recover. I am not hunting around for the best deal on a new Ninja Air Fryer.

The Unequal Power Imbalance
I was kicking myself that I had allowed another consultant to insult my intelligence. I felt shame, actually, but the power imbalance of these consultations is so unequal, that it is difficult to speak up; middle aged woman versa high powered male, stupid woman versa trained medic. No matter how many times I ask, they put the burden back on me. This is not their responsibility. It is my problem. I just have ‘to live with it.’ The Consultant agreed to do an MRI scan of my parotid gland and of my brain. Three weeks later, however, I received a letter in the post, telling me that the two scans had been cancelled and that I had been discharged from his clinic. Another door had been closed.


A Return Visit
I went back to that hospital to see an ENT Consultant about my ear-pain. He had my notes, which contained the previous surgeon’s comments. This was the fourth consultant I had asked about these CT images. That’s just because your face was lopsided in the scanner. This consultant didn’t say it with as much conviction as the previous one. He wore a Mona Lisa type smile. Behind that cryptic smile, I could see that he didn’t believe his own story.

Gaslighting Incident 4
It was at an Oral Maxillofacial clinic at an NHS Trust in Yorkshire. An MRI Neck scan had been carried out at this hospital by the ENT department. The scan had shown abnormality in my Buccal Fat Pad and retromolar region. The MRI report stated;
There is a signal change in the remnant left parotid gland. There is a plaque of increased T2 signal and abnormal enhancement in the medial aspect of the left buccal fat pad, extending superomedially into the retromaxillary region. The masticator muscles do not appear involved with this process but the abnormal region does abut the medial surfaces of both masseter and medial pterygoid. There is no evidence of periodontal disease.
The Scene
It was a high-powered surgeon, a frightened looking nurse, and me with my heartbeat in my mouth. My strategies for dealing with this fight were fading, but beneath my thud of dread, lay a veil of hope. Abnormality had been detected in the scans, so maybe this guy would take some responsibility? No chance.
The Doom of Trickery

I asked the consultant to explain the abnormality from the MRI Neck Scans. He dismissed the findings and told me that it was to do with a tooth that I previously had a one-year problem with. I pointed out that the radiology report had stated that there was no periodontal disease. He did not reply. I asked him about the masseter enlargement that had been previously detected. ‘That’s a red herring,’ he said. I brought up these MRI images on my laptop. ‘This is where I have the pain, where the red arrow is’ I said. ‘Please can you explain what this is?’



‘That is just coincidence, Felicia. It is coincidence that you are seeing that in the area you think that you are in pain,’ he said.
I couldn’t believe what I was hearing. ‘I can see that in front of me!’ I replied. ‘What I see, is where I have the pain.’
‘No, Felicia. You are choosing to see it,’ he said.
I was not choosing to see it. Can you see what I see?
‘A Gaslighter will repeatedly twist events to shift the blame to someone else, and this emotional abuse can result in victims questioning their sanity.’
How To Recognize Gaslighting and Respond to It. Angela Haupt, The Washington Post, April, 2022
Descent Into A Stygian World

The scene turned dark. I asked the nurse if she could see what I could see in the images. She looked at the floor and did not reply. The room went quiet. I asked the consultant to explain further images from the MRI scans. I explained that the highlighted area around my eye and cheek is where I have the pain. The pain in my eye and cheek is connected- I tried to explain.

Figure 1

Figure 2

Figure 3
The consultant brought these radiology images up on his computer. He proceeded to photoshop and play around with them. All of the white in figure 3 disappeared. It moved over to the right side. ‘Look, he said. It’s all gone now. It’s on the right side.’
‘But you have played about with them,’ I replied.
Each image that I presented to the consultant, he photoshopped it on his computer, so that the abnormality disappeared or moved to the other side. He was a magician. It was like sitting next to Paul Daniels. Now you see it. Now you don’t. I brought up some images which showed the left sided masseter enlargement.

Figure 4

Figure 5
He played with those images, too, so that the left masseter enlargement in figure 5 popped up on the right side. ‘See,’ he said, it shows on the right side, now. It’s just the angle of the scan.’
‘But you just manually manipulated that.’
‘No, I didn’t.’
‘Well why does the abnormality keep showing up on only the left side, where I have the pain?’ I asked.
‘I told you, Felicia. It’s coincidence.’ He slammed his hand on the desk.
‘You’re gaslighting me,’ I said.
‘I am not gaslighting you,’ he replied.
I was not only being told that I was seeing things, but the consultant was editing the radiology images in front of my eyes. It was honestly like being at a magic show.

Off Axis and Squint Angles
He told me that all of the radiology images were ‘off axis’ and ‘squint.’ According to him, all of the data is therefore unreliable. These images may be off-axis and squint, but how does that explain why over two hundred radiology images show this difference between the two sides of my face? Why does the abnormality always show up on the affected side? I do not believe that it is ‘coincidence.’ I asked the consultant about my facial asymmetry, and I showed him Figures A, B and C, along with others from that CT series.
He looked down at my iPad.
‘The quality of your iPad is s**t,’ he said. ‘If you looked at that on a better quality screen, you wouldn’t see all of that.’
‘I have looked at these images on my laptop. It is the same,’ I replied. I was so shocked by what he said, that I thought that I was dreaming.

The quality of my iPad is crystal clear. It’s not s**t. Blaming the detected abnormality, on the ‘off axis’ and ‘squint’ angle of the scan is poor, but attributing it to ‘coincidence’ and to ‘the s**t quality of my iPad,’ is scraping the barrel. I couldn’t fight him. After three hours of gaslighting, I decided to end the meeting. I was not going to get any truth out of the man. This was manipulation of the truth at its very worse.

I Felt Like I was Going Mad

I felt crazed when I walked out of that consultation. Was it me seeing things? Am I going mad? Is it my eyesight? ‘Am I nutter?’ That is how gaslighting works. It makes you question your judgement. It is a wicked and cruel misuse of power.
That was the end of the road. After ten years of attending these medical appointments, I decided that I was not going to go to any more. I was finally going to alight the merry-go-round of bullying. It was too damaging to my morale and mental health. I was going to find some self-respect and walk down a new road.
Please Stop This
This is my life. It is not a game of cowboys and Indians. I am asking reasonable questions about radiology images and symptoms which are real. I am not imagining anything. There is no history of delusion on my medical records. Answers and medical treatment are what I am seeking, to enable me to lead a normal life again.
This is a sensitive case, and I am mindful of that. I do want to make it clear that I have had enormous respect for the expertise of all of the consultants who I have seen. I have been polite and dignified with them all, and I have never doubted their clinical capabilities. What I have doubted, is the behaviour, the choices that they have made about my care or non-care, and the dismissive way in which I have been treated by many of them.
My life is of no less value than yours. If this was a relative of yours; a spouse, a lover, a parent, or a sibling, you would not stand by and watch them go through this. You would fight for them. I am no lesser of a person than any of your loved ones or relatives. Please stop treating me like this.

Gaslighting can have dire consequences leading to further harm or even the death of patients. Women are by far the group that is gaslighted the most. Medical professionals tend to see women as hysterics and do not heed a woman’s complaints or take them as seriously as men.’[2]
Recommended Articles
What is Gaslighting? Forbes Health
What is Gaslighting? Examples and how to respond.
Medical and Mental Health Gaslighting and Iatrogenic Injury
Towards a sociological understanding of medical understanding in western health care
Foot Notes
[1] Shirley Davis; Medical and Mental Health Gaslighting and Iatrogenic Injury, CPTSD Foundation, June, 2020
[2] Shirley Davis. Medical and Mental Health Gaslighting and latrogenic injury. CPTSD Journal. June, 2020.

2023-07-12 01:25
On Medical Gaslighting #1
Summary
‘Gaslighting refers to a person of power psychologically manipulating another person into questioning their own reality.’ [1] Gaslighting is a method of gaining control over someone else. It can take place in any kind of relationship but often involves an imbalance of power. People who experience gaslighting may feel confused, anxious, or as though they cannot trust themselves.[2] Medical gaslighting- According to the CPTSD Foundation, is when a medical professional dismisses a person’s health concerns as being the product of their imagination. They may tell the person their symptoms are “in their head” or label them a hypochondriac.[3]
I have been to 15 NHS Trusts over the last ten years, presenting with acute left sided facial and periocular pain, for which I have received no diagnosis or resolution. Many Consultants have implied that my symptoms are psychological, even when blood tests, scans and histology reports show abnormality. This blog post chronicles some of my experiences of being gaslighted by medical professionals. These experiences have been terrifying. They have each led me to question my own judgement and sanity. At points, I have felt like I was losing my mind.

It has been a difficult decision knowing whether or not to blog about these experiences. This is a sensitive subject and a difficult area to speak about. I have felt silenced up to this point; too afraid to speak about it. However, my blog would not be authentic without me writing about these incidents. In short, my hope is to raise awareness. I do not what has happened to me to happen to others in the queue behind me.

Gaslighting is an insidious form of manipulation and psychological control.
Psychology Today
Gaslighting Incident 1
May, 2019-It was one year after my Superficial Parotidectomy. My GP referred me to see a Surgeon at an Ear, Nose and Throat department at an NHS Hospital in London about the residual pain in my parotid gland. The surgeon organised an MRI Neck, MRI Skull base, a CT Neck scan and an ultrasound. I had all of the scans done, prior to my consultation with him.
The Scene
The Consultant had my radiology images displayed on three computer screens in front of him. An older man he was- with grey hair and he wore a red chequered shirt. I walked in and sat down. He did not discuss the radiology images with me. He said that there was nothing wrong with me and that most of my parotid gland had been removed. ‘We need to try the ‘pain psychology route,’ he told me.

He had his back to me -I remember the scene well. He was flicking through my radiology images. I was sitting directly behind him and I could see the images clearly on his screen. An MRI image flashed up. He enlarged it and moved his head closer to his computer. I could see lots of large white spots on his screen. They were big white blobs. They did not look normal.
Are they calcifications? I asked.
He turned off his computer. ‘No, they are not,’ he said. The expression he wore on his face resembled a youngster, who had been caught stealing sweets.
‘What are they? What were those white blobs?’
‘They are nothing,’ he replied.
‘They didn’t look like nothing.’
‘You must be seeing things,’ he said. ‘There was nothing there. There are no calcifications. Your problem is psychological.’
I asked him to turn the computer back on. He refused. I felt my throat tighten and my words stick in my throat. I was unable to challenge him.

The Consultant told me that what I saw on his computer screen was a figment of my imagination. I did not imagine anything. I know what I saw. They were big white globs that looked like boils. He then raised his voice and told me that I needed to see a psychologist about my pain. I walked out of the consultation. I found his behaviour too offensive.
Gaslighting means deception.
S Durbhakula and A Fortin, Turning Down The Flame on Medical Gaslighting. July, 2023
Los Angeles

I flew out to Los Angeles to see a Head and Neck Surgeon after this, to find out, a) how much of my gland remained, and b) what the residual pain in my parotid gland was. It was wonderful to be back on Californian shores. San Francisco had been my home during my twenties and this was my first time back in 18 years.
The surgeon did some scans. Firstly, he confirmed that 70% of my parotid gland remains; some of the superficial lobe is still there, the deep lobe, and there is some accessory parotid tissue over my masseter muscle. Secondly, the surgeon told me that there were still calcifications in my gland, and thirdly, he told me that my residual pain was likely being caused by my parotid gland. I came home with more knowledge and my confidence back intact.
Missing Radiology Images?

After I returned from Los Angeles, I requested the CD disk with all of the radiology images from the 4 scans that I had done at the NHS Hospital in London. On the CD disk that I received, each of the four scans were listed in rows;
CT Neck
MRI Skull Base
MRI Neck.
Neck Ultrasound
What I discovered when I looked, was a heart-thump moment. Next to each scan was a file icon. However, there was no file icon next to the MRI Neck scan. I clicked on it, and an orange sign flashed up that said; Non Image Prehensive SRSc. I clicked on that sign, and an even bigger sign came up, that said; Error decoding image. There were no radiology images for the MRI Neck scan.



I phoned the NHS Trust and asked why there were no radiology images for the MRI Neck scan. They told me that the MRI Neck images had been ‘merged with the MRI Skull base scans.’ I searched all of the MRI scans. There was no sign of the big white blobs that I saw on the surgeon’s screen. My instinct screamed out at me that all is not as it should be. The reason why the CD shows a missing file is unclear and dubious. There may well be an innocent explanation, but, I think that it is a possibility that some of the images from the MRI Neck scan may have been deleted. I will never know for sure. It will remain a question hovering over me for years to come.

Medical patients hope to feel safe, heard and cared for by doctors-but unfortunately, this isn’t always the reality. Insider.com
Gaslighting Incident 2
I was seeking answers about the CT radiology images, that I had done in Scotland in July 2021. It was my facial asymmetry, that I wanted to understand, alongside the white high-density areas on the left side of my face. There was no one who I could ask. The surgeon who had requested these scans did not give me a follow up consultation. I went to see an Oral Maxillofacial surgeon, at a private hospital in Glasgow. I asked him about the white spanner thing on the left side of my face.


‘That is your spine,’ he said, wearing a puckered expression.
‘My spine?’ I asked.
‘Yes, it’s your spine.’
It is not my spine. I could see that it was is my face. In the margin on my laptop, there is a diagram. It has a bar that moves up and down to the area of the body that you are viewing. The bar was showing the area just above my jaw.
I was too shocked to challenge him. He said it with such conviction, that I shut down. You just don’t expect it. If a cowboy tries to sell you a fake gold watch, you know that it is fake, and that he is out to snitch you. If a high calibre surgeon looks you in the eye and tells you that an image which is clearly your face, is your spine- it is disturbing. My words stuck in my throat again. I kept quiet.

I asked him about my enlarged masseter muscle and what all of the white was on the left side. He ignored my questions. He kept telling me that the images were of my spine. I don’t know what was more shocking; his lack of transparency or the conviction with which he said it to me. Writing a cheque for £175.00 was sickening. It was an exorbitant price to pay for an hour of being gaslighted.

When patients are ignored, and their symptoms not taken seriously, it can take months or years to receive an accurate diagnosis and treatment plan. Medical Gaslighting, like Social Gaslighting is a form of emotional abuse. It is traumatizing for patients, and causes confusion and helplessness.
Karen Stollznow, Phd, It’s All In Your Head; The Dangers of Medical Gaslighting. Psychology Today. May, 2022
Foot Notes
[1] Shravani Durbhakula and Auguste H Fortin. Turning Down The Flame On Medical Gaslighting. Journal of General Internal Medicine. 5 July, 2023
[2] Jennifer Huizen. Medical News Today. July, 2023
[3] Jennifer Huizen. Medical News Today. July, 2023
Recommended Articles
Medical and Mental Health Gaslighting
How To Recognize Gaslighting and Respond To It.

2023-07-06 06:47
On Gaslighting
What Is Gaslighting?
The term ‘Gaslighting,’ originated from the 1944 thriller film, ‘Gaslight’, directed by George Cukor. It starred Charles Boyer, Ingrid Bergman, and Angela Lansbury. Ingrid Bergman’s character, Paula, falls in love with the charming, Gregory Anton. Gregory manipulates and controls Paula by playing tricks on her mind, with the aim of wanting to make her think that she is losing her sanity.
He hides pictures, brooches, and manipulates her into thinking that she has lost them. Mid-film, he goes down into the basement, and messes with the gaslights. Paula hears strange footsteps in the night. She sees the gaslights dimming without being touched, and she starts to believe that she is losing her mind. Paula fights to retain her sanity, and by the end of her film, her husband’s intentions are revealed. He had been playing tricks with her mind to cover his identity, and to distract him from his criminal activities.

An Accurate Definition
The most accurate definition that I have heard of the term Gaslighting, is from British Broadcaster, Piers Morgan. He was speaking on his Talk TV Show, Uncensored, in January 2023. It was during the period that Prince Harry’s memoir- Spare was released. He was speaking about Prince Harry’s interview with Oprah Winfrey in March, 2021. During that interview, Prince Harry had said that racist comments had been made by the Royal Family, about Archie’s skin colour. There was then a U Turn- when his book, Spare, came out. Prince Harry then said, that he had never intimated in his interview with Oprah Winfrey, that there had been any racism within The Royal Family. Piers Morgan said that Prince Harry was gaslighting us. Piers defined gaslighting as;
When you lie and spin things to trick people to question their own sanity and reasoning.

Me-pedia.org describes Gaslighting as; A form of emotional abuse which involves persistently denying or refusing to accept facts. This frequently leads to the other person doubting their own experience. Victims of gaslighting may become anxious, develop depression, or become increasingly emotional as a result. This can make them more likely to be seen as having unreliable or questionable judgement, which discredits them further. Gaslighting may result in a loss of trust and isolation.
What Is Medical Gaslighting?
Medical Gaslighting is a term used to describe doctors or medical practitioners who wrongly deny a patient’s illness entirely. They tell patients that they are not really sick, or blame a patient’s illness or symptoms on psychological factors. People who experience Medical Gaslighting feel dismissed. It is certain patient groups who experience Medical Gaslighting more frequently than others. These groups are women with illnesses which do not yet have a clear diagnosis, for example, ME, Fibromyalgia, and endometriosis. These women may experience gaslighting done either consciously or unconsciously. The links below explain how Medical Gaslighting and psychologization, (the process of blaming physical problems on psychological factors) work.
Medical gaslighting – MEpedia (me-pedia.org)
Psychologization – MEpedia (me-pedia.org)

Medical Practitioner, Sarah Fraser, writes in the first article below about gaslighting between medical professionals. In the article, she makes a vital point about the subtle nature of gaslighting. She explains that Gaslighting is different from other forms of bullying. It rarely involves violent threats or aggressive insults, it is more subtle. It is a quiet form of abuse, and it often goes unseen by other witnesses. The majority of instances of gaslighting may not involve full-blown delusion or memory loss, like Ingrid Bergman’s character. However, gaslighting can have long-lasting consequences on one’s mental health and self-esteem.
The toxic power dynamics of gaslighting in medicine – PMC (nih.gov)
10 Ways People With Chronic Illness Experience Gaslighting (themighty.com)
Medical Gaslighting: 7 Signs That Help You Spot It (insider.com)
How to Spot ‘Medical Gaslighting’ and What to Do About It. – The New York Times (nytimes.com)

Recommended Articles
Sixty Seconds On Medical Gaslighting
Mind Body- Is Your Doctor Gaslighting You

2023-07-03 08:44
Questions For Radiology #3
Summary
Questions For Radiology #3 is the last of the series of my questions about my scans. In July 2021, I had a CT Neck and Bone scan done at an NHS hospital in Scotland. I did not get a follow up consultation with the Consultant who ordered the scans, so I was not therefore able to ask him any questions. Since that time, I have been trying to get answers about my radiology images. These images seem to hold valuable data about my condition, that could help me to get a diagnosis and treatment.

I am seeking answers about the facial asymmetry, that is visible in the CT Neck radiology images. There is a stark difference between the left side of my face, where I am in pain, and the right side. In addition to my facial asymmetry, I have questions about all of the white areas that appear on the affected side of my face.
I have asked four consultants about the asymmetry in these CT Neck and Bone images. Three of them have told me that the asymmetry is because my ‘head was tilted in the scanner.’ The consultants who have told me this are based in England. These CT scans were done in Scotland, so they did not actually see me go into the scanner. My head was not tilted or lopsided when I entered the scan machine. My head was central in the headrest. This is how I entered the CT scanner.


I therefore resent Consultants attributing my facial asymmetry in the CT images to my head being lopsided in the scanner. It is not true. I was central. A radiologist will not allow a patient to enter a scan machine unless their body is centralised.
Questions For Radiology
I am trying to find out what all of the white is on the affected left side of my face. It is covering my cheek bones on the affected side. Is it calcified tissue?




What could be causing this asymmetry between the two sides of my face?


The last Oral Maxillofacial surgeon who I saw, told me that where the red arrow points to in the images below is my brain. Is where the red arrow points, below, my masseter muscle or my brain? What could be causing my left-sided masseter enlargement?

CT Bone Scans
The last Ophthalmologist that I saw told me that he thought that this potential infection had only affected the soft tissue of my face and not the bone. The CT images of my bone, however, do show a difference between the left and right side of my face. In Radiology Questions #2, I asked about the thinning of the nasalis tissue. The CT bone images show a difference on the left side in this same area. Is there any damage to my bone in the sinus area?
Below are the two images showing a thinning of the nasalis tissue.


The CT bone images below definitely show a difference in this same area on the left side.





My Plea To Doctors
I have been suffering for ten years (over a decade) with this debilitating pain. Every single day of every single week, that I live, is consumed with dealing with pain. These scans definitely contain clues about what is going on in the left side of my face. I feel that I have been overlooked by the medical profession and not taken seriously. Living life again is what I desperately want, but I feel despairing that I will never find anyone who will listen and help me. I will work with any medical professional for however long it takes to find a solution. I just want answers and a remedy. If there is a radiologist, physician, Head and Neck surgeon, Infectious Diseases Specialist, Oral Maxillofacial Consultant or Otolaryngologist, anywhere in the world, who can help, please get in touch either by email; info@myfacialpain.com, X, or via the contact box. Thank you.


Useful Links

2023-06-28 06:04
Radiology Questions #2
Summary
I have suffered with debilitating left-sided head pain for ten years. For the last three years, I have also had acute pain in my left ear. My left-sided head pain and ear pain have not been investigated. The CT and MRI scans hold valuable information. These scans could help to identify a cause to my head and ear pain. I am seeking a radiologist, who specializes in Head and Neck pathology to come forward and answer my questions; to shed light on what could be causing my left-sided ear and head pain.
Ear Pain

This is a call out for radiology to answer my questions relating to my ear and head pain. I have had unrelenting pain in and behind my left ear for the last three years. I had experienced my left parotid gland push against my ear for many years. This would happen when my gland would swell and inflate. I thought that my ear pain was caused from this. However, the pain within my left ear has developed into a feeling of fullness and pressure. I have had muffled hearing, like my ear is under water. I have a consistent stabbing pain in the bone right behind my ear. Two Ear, Nose and Throat consultants have examined my ear with an otoscope, and have said that everything is ‘normal.’ This consistent pain in my ear is not normal.
The CT Neck and Bone scans show an enlarged mastoid on the affected side. I understand, from what consultants tell me, that the mastoid is sometimes bigger on one side, but it seems like a huge coincidence that the mastoid is larger on the side where I have pain in and behind my ear.
Radiology Questions

Please can a radiologist tell me if my enlarged mastoid on the left side could be contributing to my ear pain and to the throbbing pangs that I get in the bone behind my ear?


If the mastoid is not causing my ear pain, then could it be referred pain from my enlarged masseter muscle, and the abnormality in my left buccal fat pad and retromolar area? The first three images show my enlarged mastoid on the left side. The first three images below show my enlarged masseter muscle and two below show my facial abnormality, which could be referring the pain to my left ear.





Head Pain

Radiology Questions
The pain starts above my left eyebrow and it extends all the way around the left side of my head. It is a gnarly ache, which feels like hot mist under my skin. My head burns and parts of my skull throbs. There have not been any investigations into my head pain. However, MRI Neck images seem to show an enlarged nerve and frontal lobe above my eyebrow on the left. Could this nerve and frontal lobe enlargement be inflammation. Could this be causing the pain in the left side of my forehead?





Nasalis Muscle and Tissue.
There is a cross section of images from MRI Neck, CT Bone and CT Neck scans, which show a thinning of the nasalis tissue and muscle on the left side. I have asked consultants about this, but they have told me that it is just the ‘angle plane of the scan.’ If these images were all taken from one scan machine, in one hospital, on one date, I may believe this. However, these images come from different scan machines, done at different hospitals, which were done over a year apart. It doesn’t therefore stack up, that this apparent thinning of my nasalis tissue is due to ‘scan angles.’ Has the tissue or muscle on the left side of my sinus area thinned? If it has, could infection be the cause of this diminishing tissue?

My Left Lung
I have had a series of respiratory infections, since December, 2022. I still have a squeak on the left side, when I inhale. A Pulmonary Function Test (Spirometry) test has shown a possible lung function restriction. There are six images from an MRI Neck scan, which show areas of white on the left lung, which do not appear on the right side. Do these radiology images supply any information about the ongoing wheeze on my left lung?





If you are a radiologist who could help read these scans, and shed some light about what is possibly causing my ear and head pain, please get in touch with me via twitter, the message box on my website, or email me at info@myfacialpain.com

Recommended Articles
Imaging Review Of The Temporal Bone
Useful Links
Myfacialpain.com/CTNeckgallery
myfacialpain.com/mrineckgallery

2023-06-26 07:12
Radiology Questions #1
Summary
This is a call out to radiology to come forward and please help to read my CT and MRI scans. I have had unrelenting left-sided periocular pain, masseter and parotid pain for ten years. There has been no diagnosis, apart from sialolithiasis, which was identified in my parotid tissue after my partial parotidectomy in 2018. I have so many unanswered questions about the MRI and CT radiology images in my gallery. The radiology images show a stark difference between the left side of my face, where I experience pain, and the unaffected side. No explanation has been given to me about this marked difference. There is useful data in these scans, which could help me to attain a diagnosis and get the correct treatment for my condition. I am seeking a radiologist, who has an interest in Head and Neck Pathology, to answer my questions and read my radiology images.

My Periocular Pain
My periocular pain is the worst aspect of my facial pain. Orbital cellulitis was my initial diagnosis, which was triggered by a flea bite to my lower left eyelid in 2013. The area of pain that is most invasive is the left temporal artery area and around my upper eyelid and eyebrow. The region feels tight and heavy. It throbs, and my vision is now decidedly blurry in that eye. My periocular pain has worsened significantly in recent months. It is torturous enduring this pain, and I am extremely concerned about my blurry vision.
My Questions
In some of the MRI Neck images, there is visible swelling in the left temporal artery region. Could this suggest chronic temporal arteritis?




In many of the images, my left eye is smaller and less bright than the right eye. I understand that my left ptosis makes my eye small, but can a radiologist please explain why my left eye is less bright than the right one? Could it be because of reduced blood supply from the temporal arteries and vessels?


In the CT Neck images, there seems to be considerable pressure on my left eye, which is coming from all that is going on in my left cheek. Could this pressure be contributing to my periocular pain?




There has always been a connection between the pain and swelling in my eye and cheek. The radiology images show a visible connection between the two. There is a trail of white around my left eye, which extends all the way down my cheek. Could this of white be calcified tissue or infection?




My left eye does not look healthy. It is small, and it is considerably less bright than my right eye – but when I raised this with an ophthalmologist recently, he told me that it was the ‘angle plane of the scan.’ If there were a couple of images of a poorly looking left eye, I could accept this explanation. However, with so many images in my gallery, which show an unhealthy left looking eye, this does not resonate as true or accurate.

This is my body. It is my health. I am seeking answers, so that I can get treatment to recover the quality of my life. A correct evaluation of these images is the first step to me getting the right diagnosis. Please can a radiologist come forward and tell me if these scans offer any information about the cause of my eye pain.
My Left Cheek
I have acute pain in my left cheek. It starts at my zygomatic arch, and extends all the way down my cheek to the masseter and parotid area. I have had a partial parotidectomy, but a lot of my left parotid gland remains.
The MRI Neck radiology report from July, 2022 stated;
There is increased T2 signal and abnormal enhancement in the medial aspect of the left buccal fat pad, extending superomedially into the retro maxillary region. There is no suggestion of this being a primary sinus pathology and there is no evidence of periodontal disease. The masticator muscles do not appear involved with this process, but, the abnormal region does abut the medial surfaces of both masseter and medial pterygoid.
Impression;
There is abnormal signal and enhancement within the left buccal fat pad extending into the retro maxillary fat. This likely accounts for the patient’s symptoms, but it is not clear what this represents. It may be helpful to correlate with the pathology from the left partial parotidectomy. There is a focus of signal change in the remnant left parotid gland that likely represents a lymph node.
I have received no explanation re this abnormality. I did ask an Oral Maxillofacial surgeon what it was, but he attributed the abnormality to an UL6 molar tooth, with which I had a one-year problem following a faulty composite restoration. This has since had root canal treatment. The radiology report clearly states that there is ‘no sign of periodontal disease,’ so attributing the abnormality in my buccal fat pad to a painful tooth does not stack up. He also told me that it is a ‘coincidence’ that what I am seeing in these images is where I have the pain – that I am ‘choosing’ to see a problem. This does not resonate as true or accurate.

My Questions
Please could a radiologist tell me what this detected abnormality is in the retromolar and buccal fat pad region. What could be causing it? What is all the white in my left cheek? Could it be calcified tissue, or infection?





What information are these images providing re the cause of my facial pain? Is this an infection?
Conclusion
An Oral Maxillofacial surgeon recently told me that the MRI and CT images were completely normal. He said that my face looks different on each side because the images are all ‘off axis’ and ‘squint.’ If there were only a few images, which showed this stark difference between the two sides of my face, I may accept this explanation. However, there are 200 radiology images in my gallery, which show a marked difference between the two sides of my face. I cannot, therefore, accept that the difference in the two sides of my face is because the images are ‘off axis’, ‘squint’, or because I am ‘choosing’ to see a problem. I fail to understand what the object is of doing the scans in the first place, if the data is dismissed because it is all ‘off axis’ or ‘squint’ tomography?

Something is not adding up between what I see and what I am being told. I would not be in this much pain if there was nothing wrong. There is something there. I can see it – so can many others. Please can a radiologist come forward and explain what these images are showing. An accurate radiology read could help me to get a diagnosis and some long-awaited medical help.

Recommended Articles
Imaging Of Connective Tissue Diseases Of The Head And Neck
Deep Spaces Of The Head and Neck
Useful Links

2023-06-17 06:45
The Ghosting Of My General Practitioner
Summary
The jurisdiction of a General Practitioner (GP) is to treat a patient’s condition up to the point that they can, and when the problem is out of their remit, to refer the patient onto secondary care. As soon as the patient is accepted onto the caseload of the Consultant in secondary care, the responsibility for the patient’s care is with the clinical department at the hospital. The British Medical Association’s ‘The Doctor Patient Relationship Toolkit’ states; ‘Legally, health professionals have a duty of care when they assume responsibility for a patient. In secondary care, it may be once a patient is accepted onto a caseload.’

I have been with eight GP practices through this medical crisis. Every one of my GP’s has fulfilled their clinical responsibility. They have prescribed antibiotics, pain relief and anti-inflammatory medication. They have referred me to Specialists in Ophthalmology, Ear Nose and Throat, Oral Maxillofacial Surgery and Infectious Diseases. Once their referral reaches the NHS Trust, the referral gets triaged by a consultant, who either refuses to see me, or they see me once, and then send the problem back to the GP. The Consultant sometimes sends the referral onto a different hospital, but the problem normally gets batted back to the GP, who cannot treat the problem.
The refusal by the secondary care world to take ownership of my medical problem has put an enormous strain on my relationship with all of my GPs. Each time that a referral gets sent back to the GP with no resolution, the GP rightly feels that they have fulfilled their responsibility, and that they can do no more for me. I am then left to carry the burden alone. I feel angry towards the GP, when it is not their failing. It then becomes a situation of Checkmate. The GP’s hands are tied. I have to then transfer GP surgeries, because our relationship breaks down.

My Current GP
My current GP is one of the most caring and committed GP’s around. He has sent out nine referrals since he took over my care in March 2022. We are none the wiser about my condition. His first referral, which was sent to Oral Maxillofacial surgery, was rejected because the problem was ‘too complex.’ He was advised to send it to a named consultant who specialises in parotid gland disease at a Teaching Hospital. He did this in a timely manner. We did not hear anything for four months. I telephoned the hospital. I was told that my case had been closed down- that I had been discharged without being seen. The hospital did not give me any reason why they had refused to see me. They did not bother to write to my GP to tell him that the referral had been rejected. He was ghosted.

My GP then referred me to an Ear Nose and Throat (ENT) specialist re my ear pain. He received a letter, telling him that he must insist that I am seen by Oral Maxillofacial Surgery. Three Oral Maxillofacial surgery departments had refused to see me. The ENT Consultant answered none of my GP’s questions. He commented that my sinuses were clear, even though there was nothing in my GPs referral about sinus problems. The ENT Consultant shifted the responsibility. He sent the problem to an Oral Maxillofacial department at a third hospital who sent the referral back to him. Nothing was actioned. My relationship with my GP started to fracture at this point, and has since crumbled.

I struggle to understand how a GP supposed to care for a patient, when Consultants will not answer any of their questions about their patient’s condition?
My Previous GP
My previous GP in Fife had been a GP for 36 years. He had been a lifeline for me, during two national lockdowns. This guy had it even worse than my current GP. He sent referrals to ENT departments at two NHS Trusts. Both referrals were sent back to him after I had been seen only once. The ENT Consultant advised that I was seen by Pain Management. Two pain management teams then refused to see me. They said that their service was not ‘appropriate for me.’ The Infectious Diseases department then discharged me after one appointment. My GP turned to me and said; Sorry, Felicia, there is nothing more that I can do for you. My relationship with that GP completely broke down.

The British Medical Association’s ‘The Doctor-Patient Relationship Toolkit states in the section, Communicating with Colleagues, how vital it is to the patient’s care, to share information in a timely manner with colleagues who are involved in the patient’s care. It states that ‘patients who receive good co-ordination have better health outcomes and higher satisfaction rates; communication between teams involved in the patient’s care is an important component in this.’
The General Practitioner is a vital part of the healthcare chain – without them, the health network could not function. I have felt saddened by how my GP’s have been ghosted by various Medical Consultants. A GP does not send a referral out to secondary care unless they deem it necessary. Eight different GP practices would not have sent out this many referrals to specialists over the years, if there was no need. Consultants need to stop treating my GPs like pawns on a chessboard – kicking them down and taking them out. They need to start showing them respect, and start treating them as the esteemed colleagues that they are.

Recommended Articles
What Are The Responsibilities Of A General Practitioner
The Duties Of A Doctor Registered With The General Medical Council
Pressures In General Practice Data Analysis
British Medical Association; The Doctor-Patient Relationship Toolkit

2023-06-12 06:48
This Is Not Chronic Pain
What Is Chronic Pain?
Chronic Pain is when your body keeps hurting months, or even years after an injury. It can also accompany a chronic health condition, such as Arthritis. Common types of chronic pain include: Arthritis, back pain, neck pain, cancer pain near a tumour, headaches, pain in scar tissue, fibromyalgia and Neurogenic pain from damage to nerves. Injuries and disease can cause changes to your body that can leave you more sensitive to pain. These changes can stay in place even after you have healed from the original injury. A broken bone can leave you with chronic pain.
I suffer with chronic pain in both of my feet. In 2006, a plate fell off a kitchen surface and smashed on my right foot. It severed the extensor tendon. Despite corrective surgery and rehabilitative physiotherapy, I have had chronic pain in my right foot for years. I also suffer with Achilles Tendonitis in my left heel. This developed as a side effect from taking Levofloxacin, (Levaquin.) Both conditions need management and pain control. This is chronic pain. It is sustained pain after an injury. I may never be pain free. I have to control the amount of walking that I do and I have to take intermittent pain relief, and learn when to rest. Pain management is appropriate for this condition. There are many other types of debilitating chronic pain that need managing in similar ways.

Causation of Pain

Pain is often a symptom, and a cause for pain must be identified.
Aetiology; Medicine; the cause, set of causes, or manner of causation of a disease or condition.
Most diseases and conditions have a cause that don’t just need managing, but which need intervention. Without treatment, the condition worsens and the disease can create permanent damage to the body. I understand that causes for diseases are sometimes difficult to find, particularly when there is little unequivocal evidence, but ten years is a long time to be searching for a cause. I am tired of seeing Unidentified Aetiology? written on Blood Test request forms, when are sent to laboratories. They come back from laboratories with no information, even when my neutophil and White Blood Count count is raised. My facial pain is not chronic pain. I am on a quest to find an aetiology and cause for my pain. Pathology has been found in tissue histology, scans, ultrasound examinations and blood tests. There must be a cause.

Treatment Not Management
It frustrates me when Medical Consultants refer to my problem as chronic pain or ‘complex pain syndrome.’ It excuses laziness to not have to diagnose and treat the problem. Three Pain Management clinics have now refused to see me on the grounds that I was ‘not suitable for their service.’ Their refusal to accept me onto their service suggests that my condition is not one that just needs ‘managing,’ but which needs treating. Even when pain management clinics reject referrals, my case is left unresolved, and it gets closed down.
Aetiology
I am certain that the aetiology behind my facial pain is infection and residual inflammation. There have been numerous raises over the years with my neutrophils, White Blood Count, and Mean Corpuscular haemoglobin concentration, (MCHC,) as well as Haemoglobin count. These abnormal raises have never been applied in the search for a diagnosis. These blood tests are available to view on the Download page. My left ptosis, (collapsed levitator) and the malfunction and parenchymal damage found in my parotid gland is more than likely to be caused by infection or inflammation, as cancer has been ruled out. Another clue, pointing to infection being the likely cause, is that reactive lymph nodes were found in the tissue pathology of my parotid gland. Reactive lymph nodes are normally a sign that the body is fighting an infection.
What is a reactive lymph node? (medicalnewstoday.com)
If my facial pain is indefinitely dismissed as ‘chronic pain,’ I will be living with pain for the rest my life and this potential infection will eat away at my facial tissue. I do not want this to happen.

I need for Medical Consultants to stop using the chronic pain ticket as an excuse for doing nothing. It is time for the pathology that has been found to be examined, so that my condition can be diagnosed and properly treated. Ten years is a long time to be seeking answers. I need to know what can and what can’t be done, to improve things, and whether or not there is long-term damage to the soft tissue and muscles in my face.
Pathology
- A collapsed levitator, left ptosis
- Periocular pain and swelling
- Consistently raised White Blood Count, raised neutrophils and MCHC.
- Parotid gland malfunction and parenchymal damage: Sialiolithiasis.
- Masseter muscle enlargement.
- Buccal fat pad abnormality
- Calcified hardened tissue.
- Reactive lymph nodes
- Oral antibiotics quell my symptoms.
What Is This?
My facial pain is not chronic pain. I am certain that the pain that I am in, is not resulting from an injury. There is a cause to my pain, and an aetiology needs to be found. This can only be a soft tissue infection. If this is not an infection, then can someone please tell me what it is?




If anyone knows of a physician, who can help to identify a cause to my condition, please get in touch via my contact box, by email, or via twitter. Thank you.
Recommended Articles
Chronic Pain; A Review Of Its Epidemiology
The Autoimmune Aetiology of Unexplained Chronic Pain
Useful Documents

2023-06-06 08:58
On Antibiotics
Summary
I have been taking oral antibiotics for ten years, since this infection began. They are the only drugs that quell my symptoms, but they do not resolve the problem. The antibiotics subdue my facial pain, but when I come off them, my symptoms return within a few days. I have tried most of the macrolide antibiotics; Azithromycin, Erythromycin and Clarithromycin. The antibiotics that have been on repeat since 2015 are Doxycycline, 100mg, Clarithromycin, 500mg, Metronidazole, 400mg, Azithromycin,500mg. Cephalexin is prescribed intermittently, which is the most effective one that I take. I do not take any of these antibiotics at the same time. They are prescribed cyclically. The ongoing antibiotics have done no harm to my liver or kidney function, which are both checked regularly

The most therapeutic antibiotics are Doxycycline 100mg and Cephalexin, 500mg but the antibiotic that has been the most effective, by far, is oral Linezolid, 600mg. I have been prescribed it twice, for one week in 2013 and for one week in 2022. Linezolid is an Oxazolidinone antibacterial, and it is active against Gram-positive bacteria, including Meticillin-resistant Staphylococcus aureus (MRSA.) It is normally prescribed for complicated skin and soft-tissue infections, because it penetrates muscle and soft-tissue, in a way other antibiotics don’t. It is an incredible antibiotic for soft tissue infections (SSTI’s.) I have been symptom free for the one week duration, when I have taken Linezolid, but my symptoms returned when I came of it.
My Request For Intravenous Antibiotics
I have been unable to speak with a microbiologist to ask why these antibiotics only work partially. In addition, I have been unable to find out why a stronger antibiotic cannot be tried intravenously. I would love to meet a microbiologist, who could tell me why these antibiotics they quell my symptoms, when I am on them, but do not resolve the problem. I can never get past one appointment with an Infectious Diseases Physician. Questions about Vancomycin, Daptomycin, and longer-term Linezolid, are ones that I have wanted to raise, but no clinician will engage with me. I have asked for an admission to try Intravenous Antibiotics, but my request has been refused. It is difficult for me to understand why a request for an admission to try intravenous antibiotics is an unreasonable request, after suffering this long with a potential chronic infection?

Raised Neutrophils?
I have seen four Infectious Disease Consultants. They have all discharged me after one appointment, with no diagnosis or treatment plan offered. One Infectious Diseases clinician refused to see me, and sent the referral back to the GP, with no explanation as to why she would not see me. One of the hardest things for me, has been that all of these clinicians have ignored abnormal raises with my bloods over the ten years. These abnormal raises have mainly been with my neutrophils, white blood count and Mean Corpuscular Hemoglobin Concentration, (MCHC.) These are all signs of an infection being present. It is therefore difficult when these results are overlooked because they are providing valuable information about the potential cause of my condition. These blood tests are available to view in my download section.
Clinicians do not answer my questions about what the raises in my neutrophil count mean and why these antibiotics quell my symptoms, but do not cure the problem. Many of them have put forward a futile argument that the reason that I respond to the oral antibiotics is because they contain an anti-inflammatory agent.

I take anti-inflammatory tablets intermittently for Achilles tendonitis. The medications that I take are: Naproxen, 500mg, Meloxicam and Ibuprofen 600mg. These all work for my heel pain, but they have no therapeutic effect on my facial pain. If it was the anti-inflammatory agent in the antibiotics that I was responding to, then anti-inflammatory medication would subdue my facial pain. It doesn’t. I have also tried oral Prednisone, but that made my facial pain worse.
Not Placebo Effect
One Infectious Diseases Consultant, who had only met me once, and who did no diagnostic tests, told me that the antibiotics that I take are a ‘Placebo Effect.’ He said that ‘I imagine that the antibiotics are helping’- that they are dummy treatment. I do not imagine anything. If I do not take the antibiotics, my infection markers go up. My facial pain also becomes unbearable, and I become systemically unwell. I believe that the antibiotics that I take help because there is an infection that the antibiotics are responding to. It is a great shame that the first surgeon, who removed my superficial lobe, did not culture my parotid tissue. They may have found the bacteria in that tissue sample. Reactive lymph nodes were also found in that tissue, which are normally a sign that the body is fighting an infection, but again, these valuable clues have been overlooked.
What is a reactive lymph node? (medicalnewstoday.com)
The most recent Infectious Disease Consultant, who I saw, told me that Intravenous (IV) antibiotics cannot be administered when we do not know what the bacteria is causing the potential infection. He said that until the rest of my parotid gland tissue is removed and cultured, IV antibiotics cannot be administered.

There is no Head and Neck surgeon, who will remove my remaining parotid gland. I therefore struggle to comprehend why empirical IV antibiotic treatment is not worth a try. If this is a soft tissue infection, then an intervention is needed to prevent any further damage to my soft-tissue.



If anyone knows of an Infectious Diseases physician, with an interest in complex soft-tissue infections, (SSTI’S) and who may be able to help me, please get in touch.

Recommended Articles
Which Antibiotics Are Best For Skin and Soft Tissue Infections?
Practice Guidelines For The Management Of Soft Tissue Infections
Bacterial Skin and Soft Tissue Infections in Adults
Antibiotic Drugs For Treating Skin and Soft Tissue Infections.
Useful Links
Medication Template;2015-Present 1
Medication Template;2015-to Present 2

2023-06-02 07:46
A Call Out For Eric J Moore, MD
Summary
Dr Eric J Moore, is a Head and Neck surgeon, who I have been aware of for many years. There are many highly-skilled Head and Neck surgeons here in the UK. Many of them, I have consulted with. I have done the circuit in England and even moved up to Scotland to consult with the Head and Neck teams there. Unfortunately, the two NHS Trusts that I tried in Scotland both declined to help me. Sadly, I have not managed to get past one clinic appointment with a surgeon in the UK. I don’t doubt their surgical skill, their intelligence, or their calibre, but they do not want to help me.
Impasse
I have seen over nineteen surgeons across the UK. If I am lucky enough to get an appointment, they promise to do the scans, ‘discuss my case at a Multi-Disciplinary Team (MDT) meeting,’ and then promise to find a ‘way forward.’ Two weeks later, I receive a letter telling me that the scans have been cancelled, or that I need to be seen by a different department at a different hospital and that I am discharged from clinic. One Head and Neck surgeon in Scotland, who I waited four months to see, promised to find a way forward at my initial consultation, but proceeded to go silent on me for eighteen weeks. I wrote to this Consultant four times asking for a follow up consultation, but I received no reply. I never heard from him again.

It is soul-destroying knocking on door after door that will half-open, and then which slams shut in my face, or which does not open at all. I would be delighted to see any surgeon in the UK, but the Head and Neck medical teams in the UK seem to have shut its door on my case.

Eric J Moore, MD
I have been aware, for many years, of a gifted Head and Neck Surgeon in the USA. His name is Dr Eric Moore. He practices at the world-renowned Mayo Clinic in Rochester, Minnesota. I stumbled upon a You Tube video of him one night. It was around 3.00am. I had been unable to sleep because of my facial pain. I clicked on a video link of him, in which he speaks about his passion for Head and Neck surgery.
Dr Eric Moore has devoted 25 years, nearly half of his life, refining his surgical skills. He performs Trans Oral Robotic surgery for minimally invasive throat cancer as well as facial reconstruction. His passion is for parotid gland surgery. He speaks about performing this surgery with precision and to minimize what he calls ‘the surgical footprint of the surgery.’ Below is the video, that I stumbled across of this awesome guy!
His love for this field of medicine is palpable. I would trust this surgeon with my face –100%. It is unclear is he performs Head and Neck surgery solely for cancer patients, or whether he also deals with benign disease. If anybody knows whether Eric J Moore, MD sees patients with benign disease or whether he sees solely oncology patients, please can you get in touch, either via email or twitter.
I would absolutely love to meet this guy. If Eric Moore was willing to see me, I would be on the first plane out of Manchester airport to Minnesota. I am not that great at DIY, but if no planes were flying out that day, then I would make my own wings, and fly to Minnesota myself.

Recommended Articles
Useful Links
Dr Eric Moore, MD- On Parotid Tumour
Mayo Clinic; Parotid Tumour Recovery Guide.

2023-05-29 10:10
On Revision Parotidectomy
Summary
The outgoing Head and Neck surgeon has left me in an uncompromising position. He has removed some of my superficial lobe, but not all of it. He has left a huge amount of my parotid gland in- about 70%, I have been told. A scan done one year after my operation showed that there is still some of the superficial lobe in, the deep lobe is all there, and there is some accessory tissue over the masseter muscle. The duct is still attached to the remaining gland. My surgeon did not cut my duct and tie it up. Below is a link to the MRI Neck images, which show how much of my left parotid gland remains.
My Situation 5 Years Since Surgery
We know that there is pathology in my salivary gland. It was found via ultrasound scanning and sialography at a London Teaching Hospital in 2015 that my parotid gland was not functioning properly. Mucous plugging and a thickening of saliva was detected, and was treated with ongoing sialendoscopies and steroid therapy. The histology of my parotid tissue from 2018 showed abnormality. It showed numerous calcifications, dense secretions in the ducts, and reactive lymph nodes. The parenchyma was sialolithiasis.
My remaining parotid gland is rock hard. It swells when I eat and drink, and it presses against my left ear. It constantly burns and the duct pinches. I did think that once parotid tissue had been removed, that the remaining gland would die, but this has not been the case. My gland still producing saliva, but it is still not functioning.
Because of my post-surgical paralysis, I am now untouchable to any incoming Head and Neck surgeon. I have seen over nineteen Head and Neck surgeons in the UK. They have all refused to remove the rest of my parotid gland because of the risk of further paralysis.
I appreciate that no surgeon wants to perform a procedure that could cause further paralysis. I also understand surgeons saying that they will only perform parotid gland removal unless there is a tumour there, as revision surgery is largely reserved for oncology patients, but, it is not healthy to have a salivary gland which is not draining saliva away, and which is calcified. There is no tumour, but benign abnormality hurts. I am in constant pain and I have no quality of life. It feels like there is an animal inside my cheek, which is constantly moving and burning.

My Plea To Head And Neck Surgeons
I have had many years to reflect on the risks involved if revision surgery were performed, the worst being permanent facial nerve damage. I have been living with incessant pain now for ten years, which is largely being caused by my damaged parotid gland. That is a decade of my life gone, and a decade during my prime years. During these ten years, my vocation, my relationships, and my ability to function normally have all been severely impacted. Both of my parents died at 78 years old. If I am to follow in their genetic footsteps, I have 30 years left of my life. I cannot live with this pain for another thirty years. I may have the ability to smile now, but I rarely do, because of unrelenting pain.
If I was left with temporary nerve palsy again, I recovered before. I would recover again. I know what to do now with eye taping etc. If I was left with facial nerve palsy for the rest of my life (and this may not happen with a pair of careful hands,) I would still have a better quality of life than what I currently have. Yes, it would be difficult. I would have to adapt, but I would cope. It is my body, and it is my life, that I am trying to desperately recover, and I would choose facial nerve palsy over this incessant pain.
Pathology Versa Chronic Pain
I find it frustrating that Head and Neck Surgeons do not hear me when I tell them that there has been a sustained improvement and reduction in my facial pain levels, following my superficial parotidectomy in 2018. I am able to eat and drink with less pain, and I don’t feel so systemically unwell. However, surgeons have told me that removing the rest of my parotid gland would make things worse.
Their argument implies that my pain is postsurgical pain. There is no way that the pain in my parotid area is post-operative pain. It is now five years since my operation. If I did have ‘complex pain syndrome,’ or pain related to scar tissue, then I can understand how further surgery would make things worse, but my pain is not coming from previous surgical injury. How do I know this? The pain that I have in the parotid area is the same gnarly pain that I had pre-surgery, just less of it, because some tissue has been removed. I can still feel the gland swelling and inflating when I eat and drink, and I still feel the duct pinching. Pathology was found in my parotid tissue and glandular malfunction was detected prior to surgery. We know that there is abnormality there.
Conclusion
I am certain that my residual parotid pain is coming from pathology in the remaining parotid tissue, and the thinned parotid duct. The case that I have been presenting to surgeons, but which does not get heard is, that if the removal of the parotid tissue in 2018 reduced the volume of pain that I had, then surely, removing the remaining tissue, and tying up the duct would surely be an amelioration. It may not resolve my surrounding periocular, ear or head pain, but it would solve one large piece of the puzzle.

I just cannot get heard with this one.

Recommended Articles
Factors Associated With Facial Weakness Following Surgery For Benign Parotid Disease
Patterns of Facial Nerve Palsy During Parotidectomy
House-Brackmann Facial Nerve Grading System
Antegrade Versus Retrograde Facial Nerve Dissection in Benign Parotid Surgery

2023-05-26 06:22
Parotid Gland Surgery #2
My Surgical Experience
I was unlucky with my surgical experience. It is difficult when seeking out a surgeon, to know how many parotidectomies they have performed. My experience of seeing Head and Neck surgeons over the last ten years, is that some surgeons in Ear, Nose and Throat, specialise in thyroid and parathyroid surgery. They have not always done a lot of parotid gland removals. In Oral Maxillofacial surgery too, some may have done skin cancer surgery, dental surgery and cosmetic facial reconstruction. They may not always a huge amount of parotid gland surgery. Whether it is cancer or benign disease, it is important to ask your surgeon how experienced they are with this surgical procedure.
I had a superficial parotidectomy in April 2018. My surgeon decided to do the operation without doing a scan first. He went in blind, and operated with no imagery at his disposal, only the knowledge that I had been having endoscopies to treat glandular malfunction.
I feel enormous remorse that I allowed this to happen. If my surgeon had done a scan of my parotid gland beforehand, he may have seen the pathology in its entirety, and if he had not been confident to remove the whole salivary gland, he could have referred me to someone who could. I may now be in a very different position.
My surgeon told me that he would not remove the entire salivary gland because he said that if he were to remove the deep lobe as well, the risk of permanent facial nerve damage was too high. I did expect, however that when he agreed to do a superficial parotidectomy, that the entire superficial lobe would be removed, and that the parotid duct, which my surgeon knew was thinned, would be cut and tied up. This didn’t happen.
I signed a disclaimer before surgery: I accepted the risk of facial paralysis, and the risk that I may still have symptoms with the remaining deep lobe. Post surgery, I knew the minute that I woke up in the recovery room that I was paralysed. Once they had removed the oxygen tube from my mouth the registrar, who was standing at the end of my bed, was shouting at me;
‘Blink, Felicia, wrinkle your nose, blow air into your cheeks.’
I couldn’t do any of it – and when I tried to speak, my mouth was drooping downwards. It was a shock- I won’t lie. I thought that the risk of paralysis was rare, but if it was, then I was one of the rare ones. I did not see my surgeon after the operation. His registrar, however, told me that they had tested the facial nerve, and that it had been preserved and was functioning fully. They were confident that my facial nerve palsy was temporary and that it would recover. My facial nerve paralysis got progressively worse during my three day stay on the ward, despite IV steroids being administered.
All five branches of the 7TH Cranial nerve were affected. My facial nerve damage meant that I could not shut my eye, smile, wrinkle my nose, or raise my eyelid. My mouth was also drooping. I did have some movement – I could still speak, eat and drink, but I did score IV on House-Brackmann scaling, which is moderate to severe palsy.




This was me post surgery. Go easy on me, please. I know I look like The Joker!
Recovering My Facial Function
I found a gifted physiotherapist at The Lindens Clinic, which is a Specialist Facial Rehabilitation Centre & Nerve Injury Rehabilitation Centre in Greater Manchester. She worked with me for five months. She gave me gentle exercises to do, which focused on raising my facial tissue and muscle upwards, and she taught me how to tape my eye shut at night, which I had to do before going to sleep every night.
It was a wonderful day when my facial function started to return. I was on holiday on the Greek island of Kos, where I spent a week in the sleepy town of Kefalos. Taping my eye and doing my physio exercises daily were part of my rehabilitation. I spent the time swimming in the Mediterranean Sea, eating lamb chops and chips and relaxing in the sunshine. On my last night, I was sitting out on the veranda where I was staying, with Martin and Belle, a couple who were staying next door. We were drinking Ouzo and watching the brilliant pink and red sunset. Martin told a joke. It made me laugh and without realising it, I smiled.
‘Your smile is coming back,’ Belle said.
After returning from Greece, my paralysis progressively lifted. Within five months, I had recovered my full facial function.



My facial function recovery took five months in total. That is quite quick. It takes many patients up to twelve months to recover. The only lasting damage has been a mild astigma in the affected eye. It becomes easily dry, and I have slightly blurry vision. This is managed with Carbomer eye gel, to keep my eye moist, and reading glasses.
Living With Facial Nerve Palsy
Living with facial nerve palsy is tough, because you cannot express emotion. You cannot smile or laugh, nor can you express when you feel sad or frightened – and you lose your looks. I missed my lovely smile, and when I looked in the mirror, it was tough because I could not recognise myself. Children on trains and buses asked what is wrong with her face, Mummy? It was upsetting, but I learnt to say, I have not had a stroke. It is just facial nerve damage, when I met anyone new.
Facial nerve palsy does not physically hurt and it didn’t actually affect the quality of my life. I still saw my friends and the essence of my character still came through. Feeling like a different person is part of having facial nerve palsy, but people said that I was still the same person. I was still able to eat, drink and articulate. Writing is a vital part of my life, and I could still write. I went on to self-publish my first novel even with facial nerve palsy.
I was delighted when my facial function returned. It was wonderful to be able to smile again, but when I look back at the five months that I was paralysed for, it was not all bad. I mostly remember how kind and compassionate people were towards me in public places; on buses, in shops and in hospital waiting rooms etc. People went out of their way to help me. That period in my life, when I had facial nerve palsy, it reminded me of the inherent goodness of people.

Recommended Articles
Factors Associated With Facial Weakness Following Surgery For Benign Parotid Disease
House-Brackmann Facial Paralysis Scale
Resources

2023-05-23 10:55
Parotid Gland Surgery #1
The Parotid Gland
The parotid gland consists of two lobes; the superficial lobe and the deep lobe. The parotid duct is a salivary duct that emerges from the parotid gland, and it runs along the lateral side of the masseter muscle, and opens into the vestibule of the mouth, between the cheek and the gums, at the parotid papilla, which lies across the second upper molar tooth. It deposits saliva into the mouth.

The Seventh Cranial Nerve
Parotid gland removal is one of the most challenging and complex procedures in Head and Neck surgery. The seventh cranial nerve, which stimulates all of our facial movement, runs directly through the parotid gland. The cranial nerve arises from the brain stem and extends posteriorly to the abducens nerve and anteriorly to the vestibulocochlear nerve. It courses through the facial canal in the temporal bone and exits through the stylomastoid foramen after which it divides into branches at the back edge of the parotid gland.[i]

A portrait of woman’s face, showing the seventh cranial nerve, and the different branches, which run through the parotid gland.
The Facial Nerve Branches.
All of our facial movement is stimulated by the cranial nerve: the muscles of facial expression, the left forehead wrinkle, left eyelid closure and movement of the left half of our face including our nose, mouth and eyebrows. The five branches of the 7th cranial nerve are;
- The temporal branch –innervating the muscles in the upper part of the face.
- The zygomatic branch- innervating the middle part of the face.
- The buccal branch- innervating the cheek muscles, including the buccinators muscle.
- The mandular branch- innervating muscles of the lower part of the face.
- The cervical branch- innervating the muscles below the chin and the platysma muscle.[i]
The 7th cranial nerve is miniscule, and when a surgeon performs either a partial or a complete parotidectomy, they have to carefully isolate the facial nerve, so that it can be preserved during surgery. This is an intricate procedure – even with the most careful pair of hands, the facial nerve can get accidentally nipped or cut. If there is a tumour over the nerve, then the nerve has to be cut, but the patient is made aware of this before surgery.
Surgeons will test the facial nerve during surgery to check its functionality. However, f it gets nipped, the patient can end up with facial nerve damage, either permanent or temporary. Even if the nerve is fully preserved, the patient can still be left with temporary facial nerve damage, which can be caused from bruising or pulling of the nerve.
Minimally Invasive Procedures.
Due to the complexities of parotid gland surgery, salivary gland removal is reserved as a last resort when treating salivary gland disease, such as Sialadentis and parotitis. In order to preserve the facial nerve, minimally invasive procedures are tried first. Sialoendoscopy is a therapeutic procedure, which is used to remove salivary gland stones and treat salivary gland inflammation. Ductoplasties are another minimally invasive procedure to treat benign salivary gland obstruction. These can repair a damaged duct, which has thinned, (stenosis), by using angioplasty balloon. Both of these minimally invasive procedures were tried in 2015. I found the saline irrigation of my gland to be therapeutic. In summary, the relief that these procedures brought me, was only short-term. That is why I had a superficial parotidectomy in 2018.

This image shows a clinician carrying out a sialendoscopy on a patient, who suffers with parotid gland disease.
Recommended Articles
Complications Of Surgery Of The Salivary Glands
Treatment Of Complications Of Parotid Gland Surgery
Intraoperative Facial Nerve Monitoring In Parotid Surgery
Foot Notes
[i] Myckatyn TM, Mackinnon SE; A Review of Facial Nerve Anatomy. Semin Plast Surg. 2004, Feb. A Review of Facial Nerve Anatomy- PubMed (nih.gov)
[i] Dominika Dulak; Imama A. Naqvi. Neuroanatomy, Cranial Nerve 7 (Facial); National Library of Medicine National Centre for Biotechnology Information. Stat Pearls Publishing; 2023, January.

2023-05-22 09:34
My Facial Pain
Summary
I have been suffering with left sided facial pain for ten years. My pain relates to the soft tissue and muscle inside my left cheek, from my zygomatic arch all the way down to my jaw. The most agonising area is the masseter and parotid area, which is rock hard, burning hot, and it inflates and swells constantly. The images below show exactly where I experience most of my facial pain: in the bottom corner on the left side.


Parotid Gland Histology
In 2015, a salivary gland unit at an NHS London Hospital found that my left parotid gland was not working properly. Obstruction and mucous plugging were identified and was treated with repeated sialendoscopies and Corticosteroid irrigation therapy in the gland. These only brought me short term relief. In 2018, I had some of the superficial lobe of my gland removed. The histology showed dense secretions, numerous calcifications and reactive lymph nodes. The parenchyma was sialolithiasis.

My Residual Parotid Tissue
I have experienced an improvement following the removal of some of my parotid tissue, but a lot of my gland remains, and my parotid duct has not been cut and tied up. There are four images in my gallery on the MRI parotid page, which show how much of my left parotid remains.
A scan done one year after surgery, showed that some of the superficial lobe still remains, as well as the deep lobe and some accessory parotid tissue over the masseter muscle. Whilst residual salivary gland does sometimes shrivel up and die after surgery, mine hasn’t. I have a large amount of a malfunctioning parotid gland alive and kicking in my face. Every time that it pulls and inflates, it feels like there is an animal, writhing in my face.

Buccal Fat Pad Abnormality and Masseter Enlargement
Recent MRI and CT scans have shown left masseter muscle enlargement and left buccal fat pad abnormality, which have not been explained to me or followed up with any remedy or treatment.



The top two images show the buccal fat pad, and the image below shows my enlarged masseter muscle. Many surgeons have offered me Botox injections, which I have refused. I have refused Botox injection because no cause has been identified for my masseter enlargement, buccal fat pad abnormality, parotid disease or periocular pain. Botox injections could therefore make things much worse. If infection if the cause, then the problem needs treating at its source. We need to know what we are treating.
I am on a quest to find diagnosis and a cause to my facial pain.

My Quest To Find Answers
- There are over 100 radiology images in my gallery, which show a stark difference between right side, (the normal side) and left side of my face. I have received no explanation re what this asymmetry is. When I ask consultants to explain these scans, they tell me that it ‘is just the angle of the scan,’ but I do not see how the asymmetry that shows in all of these radiology images can be due to the ‘angle of the scan.’
- I asked an Oral Maxillofacial surgeon recently about what the two MRI images below show. He told me that ‘it was coincidence that what I am seeing on the scan is where I have the pain.’ I do not believe that it is a ‘coincidence’ that I can see something wrong in the exact place where I am in pain. What do these images show?


- What is the abnormality in the Buccal Fat Pad?
- What could the white areas on the left side of my face? As the histology from my parotid tissue showed hardened tissue, could the white be calcified soft tissue?


- A scan done in 2019, showed that there is still some accessory parotid tissue over my masseter muscle. This report is available to view in my download section. Could my masseter enlargement be caused by residual parotid tissue disease, or could the masseter muscle now be damaged? Below is an image of my left masseter muscle. Further CT and MRI images are available to view in my gallery.

- What are the white areas, which are visible on the MRI Left Enhancement page in my gallery?
- Left Enhancement – My Facial Pain
Seeking A Prognosis

I am seeking a diagnosis and treatment for my facial pain. Receiving a prognosis is also vital. I want to know if there is irreparable damage to my soft tissue and muscle. I also want to ascertain whether or not this is now treatable, or if it been left too long, to now treat? Ultimately, I am looking for a Head and Neck surgeon, who could remove my remaining parotid gland safely.
Getting Past One Appointment
I can never get past one clinic appointment with Head and Neck surgeons in Oral Maxillofacial Surgery and Ear, Nose and Throat departments. Numerous GP’s and clinicians have referred me to over forty clinics at fifteen different NHS Trusts. Secondary Care clinics either reject or close down my GP’s referral. Consultants will sometimes send it on to another hospital, who then bat it back to the GP or referring consultant with no outcome. Or consultant’s see me once, twice maximum, and then discharge me with no treatment plan. It is like being on a merry-go-round. I feel exhausted.
No-one seems to want to deal with my medical problem, because it is too ‘complex.’ However, what Consultants forget is that there is a human being under all of these scans and blood tests, a human being who is suffering, and who has completely lost the quality of her life because of enduring pain. This person wants the quality of her life back.

If anyone knows of a Head and Neck Surgeon, who has an interest in benign disease, please get in touch. You can contact me via email; info@myfacialpain.com, on Twitter, or via the contact box, on my Contact page. Many of the surgeons who I have seen, treat solely oncology patients. I am on a quest to find a Head and Neck Unit which diagnoses and treats benign disease. There is no tumour in my left parotid gland, ear or head. This is likely, long-term infection and inflammation with potential soft tissue and muscle damage.


2023-05-09 09:12
My Left Sided Head Pain
Summary
Left sided head pain is something that I have bene suffering with for the whole duration of this medical episode. It is a severe throbbing pain around the left side of my head. The pain extends from my left eye and temporal region through to my ear and all around the left side of my head. It feels like a nail is being drilled into the middle of my skull. The pain has worsened significantly in the last two years. The prominent area of pain is the bone immediately behind my left ear. There is a stabbing pain and dull ache there. I have a throbbing pain at the top of my skull. I have raised this with many different ENT specialists, but they have not investigated it, or answered any of my questions.

There is a gnarly pain on the left side of my forehead, just above my eyebrow. There is a constant dull ache there most days. In the MRI Neck images, the front lobe of my head and my nerve on the left side of my forehead, is bigger than on the right-hand side. If I raise this with any specialist, they say it is just ‘the angle of the scan.’ This does not resonate as true, as in my gallery, you can see more than six or seven images showing this enlargement on the left side above my left eyebrow. Below are examples of the images that I refer to.




When I take oral antibiotics, the pain around the left side of my head subdues, especially the stabbing pain in the bone behind my ear. However, when I come off the antibiotics, the pain returns.
Questions About My Left Sided Head Pain
- What could be causing this pain?
- If this is a soft tissue infection, could there be infection around the soft tissue of my head?
- Is it possible that the pain around the left side of my head could be caused by mastoid or temporal bone enlargement?
- Is it a skull-based otolaryngologist who deals with this?

Methicillin-resistant Staphylococcus aureus bacteria.
My Concerns About My Head Pain
The pain on the left side of my forehead is not a migraine nor a headache. It is not separate from my facial or peri ocular pain. There is a similar quality about it to my facial pain. The pain feels like there is burning hot mist under the skin. My head throbs, all around the left side. I have not had my head pain properly investigated with an MRI scan. The pain is worsening, particularly where the bone is, right behind my ear. I am extremely concerned about this.
The last Ear Nose and Throat Consultant who I saw, said that he thought that my head pain could be to associated with my temporal bone. At the time, he told me that he needed to take a careful look at my temporal bone. However, he did not carry out any investigation of my temporal bone. He sent my case on to Oral Maxillofacial surgery.
Temporal Bone
Both my head and ear pain have both significantly worsened in the last year. I currently have no ENT consultant to speak about it with. It would be useful to have my temporal bone and muscle looked at. This is because they are both situated close to the zygomatic bone, right under my eye, where I experience acute pain. They are also not far from the Maxillary and mandible regions, where pathology has been found, and where my medical problems are originating from. As these spaces are all so closely linked. I am wondering whether the cause of my head pain is the same cause behind my eye and facial pain?


Could this be a peripheral soft tissue infection?
I am looking for a skull-based otolaryngologist who specialises in the temporal bone and the mastoid. If you are an Ear, Nose and Throat clinician, who specialises in this, please get in touch with me via Twitter @myfacialpain or email me at info@myfacialpain.com.

Photo by Daniel Andrade on Unsplash
# Head pain. # Temporal Bone. #Temporal Bone Enlargement # Mastoid. #Mastoiditis. # Skull Base Otolaryngology. #Skull-based Otolaryngologist. #A Quest To Find Answers. #My Facial Pain. #Neurosurgeon. #Seeking medical help. #Seeking a diagnosis. #Seeking Medical Treatment.

2023-05-04 04:05
My Periocular Pain
Summary
My medical problem began with a diagnosis of Orbital Cellulitis in 2013. This was triggered by a flea bite to my lower left eyelid. Periocular pain and swelling were my initial symptoms. They have remained chronic symptoms, which have worsened over time.
Acute pain in my lower eyelid was eradicated in 2014 with a one-week course of Linezolid. I have been able to only get the drug once in 2022. Since 2014, persistent pain and swelling around my upper eyelid, eyebrow, and the area around the temporal artery area has been persistent and acute.
In 2014, the levitator on my upper eyelid collapsed. I was diagnosed with a left ptosis, which I was told needs correcting. However, a Professor of Ophthalmology told me that until all of my symptoms have abated, it is not safe to perform the surgical correction of my left ptosis.
My Left Ptosis



My Symptoms Now
I have a gnarly pressing pain around my left eye. There is a constant feeling of pressure around my upper eyelid and eyebrow. The area burns. I have severe pain around my left temporal artery, which feels tights and throbs constantly. The throbbing pain in my temporal artery region has worsened in the last year. It is now so bad, that it keeps me awake at night. My entire periocular area burns. It feels like I have hot mist under the skin. I am most worried about the pain around my temporal artery because of the blood vessels in that area. My vision in my left eye has also become blurred in the last two years. I now wear reading glasses.
Eye and Parotid Connection
My periocular pain is connected to the pain in my masseter and parotid area. It extends like a rainbow arch, down from my eye, through to my zygomatic arch and through my left cheek, to the region adjacent to my jaw. Below are two drawings that I did for a Medical Consultant in 2014 and 2016. They are supposed to illustrate that my eye pain and my parotid pain are connected. They are not separate problems.


This is a picture that I drew for a consultant in 2014. It shows the parotid/masseter area, inner cheek, and eye pain are all interconnected. I was trying to show that they are not separate problems.
In my drawings above, which I did in 2014, I highlighted the areas on the left side of my face where I experience pain. That same area is mirrored in the MRI scan images below. It is clear from the scan images that all is not well with the soft tissue of my left eye and cheek, and that the problem with both my left eye and cheek is connected.



When I take oral antibiotics, my periocular pain subsides, but when I stop taking them, my pain returns. I have seen seven different ocularplastic surgeons in Ophthalmology clinics, at NHS Trusts in England. They have each discharged me after one appointment. I have not received a diagnosis or answers re my orbital pain (apart from my ptosis diagnosis.) In spite of raises with my neutrophil and White Blood Count, no clinician has identified or named infection as the cause.
‘The Issue Is With The Tissue.’
I did get an acknowledgement from an Ophthalmologist, that this is a problem with my soft tissue. The Ophthalmologist who I most recently saw, said that the ‘issue is with the tissue.’ I asked him about the above scan images of my left eye, but he told me that ‘everything is normal.’ The pain around my eye does not feel normal. He said that it is just ‘the angle of the scan.’ This does not resonate as true. There are too many scan images from different hospitals and done on different dates, that show the same thing.
My Questions About My Periocular Pain
In the MRI Neck images below, there is swelling in the area around my left temporal artery, where I have acute pain. Could this swelling indicate inflammation of my left temporal artery, or chronic temporal arteritis? Would IV antibiotics improve things if infection is the cause? Or can steroids treat it?



In the one MRI and two CT images below, there is a heap of white surrounding my left eye and down the left side of my cheek, where I experience most pain.



Calcified Tissue?
The histology from my superficial parotidectomy showed calcified, hardened tissue. This report is available to view in my download section. Many of the radiology images, available to view in my gallery, show a lot of white on the affected side, particularly around my left eye. Could the white areas that surround my left eye be calcified soft tissue? I am wanting to find out if this can be treated, or whether it is irreparable damage?
If the white areas are not calcified tissue, what could they be?
If anyone knows of an ophthalmologist, who specialises in ocular plastics and pathology of the temporal arteries, who could help cure my chronic periocular pain, please get in touch by Twitter, email;info@myfacialpain.com or via my contact page.

Photo by Priscilla Dr Preez on Unsplash
#Periocular pain. #Ptosis. #Ocularplastics. #Ocularplastic surgery. #Temporal Arteritis. #Temporal Artery pain. #A Quest To Find Answers. #Seeking a diagnosis and medical help. #Intravenous Antibiotics. #Soft Tissue Infection. #Antibiotics. #Calcified tissue. #Hardened tissue.

2023-05-04 04:02
My Ear Pain
Summary
In January 2020, seven years into this episode of facial pain, I developed persistent pain in my left ear. I had felt pressure against that ear for many years – this would occur when my parotid gland would swell and push against it. The parotid gland is situated right next to the ear, so I naturally suspected that my ear pain was being caused from my swollen parotid gland. However, as new symptoms have developed, I have been forced to explore other causes for my left ear pain.
The pain in my left ear is persistent and worsening. My ear feels full and my hearing is muffled. It feels like my ear is under water. There is a constant feeling of pressure. I have had many episodes of pulsatile tinnitus; a loud heartbeat sound in my ear. Questions have arisen as to whether these symptoms are caused by mastoid enlargement or temporal bone involvement. This question arises about mastoid involvement because of the pain in the bone behind my ear and because the CT images show an enlarged mastoid space on the left side. I have asked many Ear Nose and Throat consultants what the cause for my ear pain could be. I have received no answers.
Eustachian Tube Dysfunction
On the website hopkinsmedicine.org, it explains that the symptoms that I have; prolonged pain and pressure in the ear, a sense of fullness, muffled hearing and a popping sound can be symptoms of Obstructive Eustachian Tube Dysfunction.
Eustachian Tube Dysfunction | Johns Hopkins Medicine
Recent research that I have done, has taught me that the Eustachian tube, which equalizes pressure between the atmosphere and the middle ear, extends from the middle ear through the parapharyngeal space to the upper part of the throat, just behind the nose. The parapharyngeal space, where the Eustachian tube is located, is behind the masticator space, where pathology has been found. Lateral to the parapharyngeal space is the parotid space, where most of my problems originate. Below is an illustration of the eustachian tube.

My Questions
As these fascial spaces are so closely linked, if infection is the underlying cause for my facial pain, I am wondering if it possible that the infection has moved from the parotid space to the Eustachian tube, or that the fluid build-up from my parotid gland has moved through the fascial spaces into my ear, causing damage to the Eustachian Tube? Or could my enlarged mastoid be causing my ear pain?



Could my left ear pain be caused from pressure from the left masseter enlargement and mastoid combined?

Pressure and Fullness in Ear
I have pushed for answers from four different Ear, Nose and Throat consultants, but I have received no answers. Two recent Ear Nose and Throat (ENT) Consultants both unfortunately discharged me from clinic after one appointment. They examined my ear with an Otoscope and told me that; ‘Everything is normal.’
The pain in my left ear is not normal; the pressure, the feeling of fullness, and the muffled hearing are not normal. I have never had a CT or an MRI scan done solely of my ear, or temporal bone, which was named by one ENT consultant as a positive cause. Head and Neck surgeons usually request a CT or MRI Neck scan. I feel that it would be useful for my left ear to be properly investigated in order to find out what is causing this pressure and feeling of fullness.

Is This Referred Pain from My Parotid?
I am not currently under the care of any ENT Consultant. It is therefore not possible for me to speak to a specialist about my ear pain. The most recent ENT consultant who I saw recommended that I see a skull-based Otolaryngologist about my ear pain, but he also said that my medical problem is the responsibility of Oral Maxillofacial surgery. He said that he thinks that my ear pain is referred pain from my parotid pathology. Is it possible that my ear pain is coming from the residual parotid gland?

It seems possible that that my medical problem straddles between Ear Nose and Throat, Oral Maxillofacial Surgery and ocular plastics. The fascial spaces are so closely linked. The areas around the eye, head and ear are all within such close proximity. I believe that it would be beneficial if these disciplines were able to work together for this to get successfully diagnosed and treated.

My left ear pain is getting progressively worse. The most prominent symptom is the pressure and the feeling of fullness. I need to see an Ear Nose and Throat Specialist with whom I can get past one clinic appointment. It would be wonderful to find a consultant who will engage with me. I am seeking a skull-based Otolaryngologist, who specializes in the mastoid and temporal bone. If anyone knows of one please get in touch with me by Twitter or email.

Photo by Courtney Hedger on Unsplash
#Earpain. #Fullnessinear. #PulsatileTinnitus. #Mastoid. #MastoidEnlargement. #Mastoiditis. #Temporal Bone. #TemporalBoneEnlargement. #Skull-baseOtolaryngology. #EustachainTube. #EustachianTube Obstruction. #EustachianTubeDysfunction. #PressureinEar. #Seekinghelp. #Seekingadiagnosis. #Seekingmedicaltreatment. #BenignDiseaseofTheHeadandNeck. #HeadandNeckSurgery. #JohnHopkinsUniversity.